Risperidone: Use, Side Effects, Mechanism of Action
Medicine Details
What Is Risperidone
Risperidone represents a significant advancement in antipsychotic pharmacotherapy, belonging to the second generation of antipsychotic agents commonly referred to as “atypical antipsychotics.” This medication has fundamentally transformed treatment approaches across multiple psychiatric conditions since its introduction, offering improved efficacy profiles and reduced extrapyramidal side effects compared to traditional first-generation antipsychotics
. Its unique pharmacodynamic characteristics and broad therapeutic applications have established it as a cornerstone medication in modern psychiatric practice.
Pharmacological Classification
Risperidone is classified as an atypical antipsychotic or second-generation antipsychotic (SGA). Within this category, it demonstrates characteristics of a benzisoxazole derivative and functions as a multireceptor antagonist with partial agonist properties at certain receptor subtypes. The compound is structurally distinct from both phenothiazine and butyrophenone antipsychotics, contributing to its unique clinical profile.
How Risperidone Works
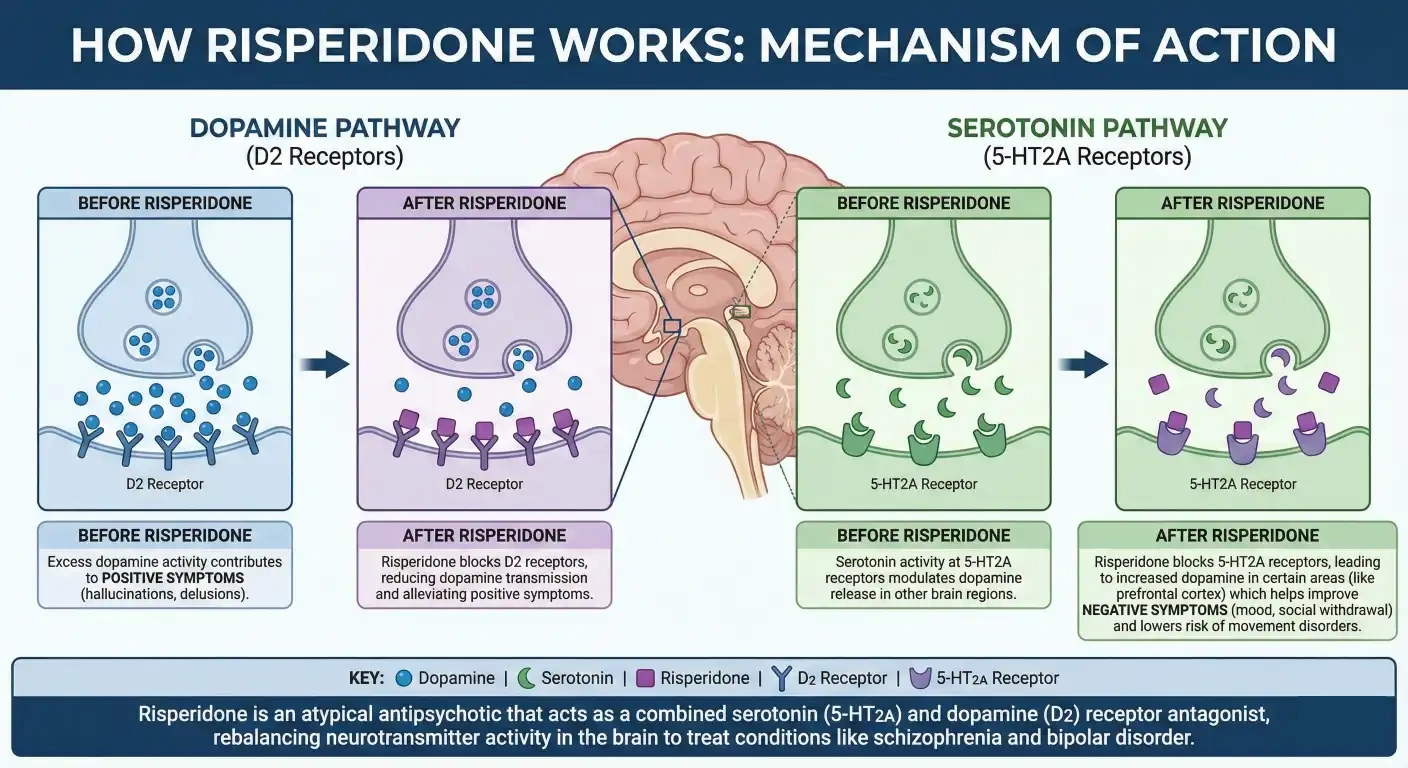
Risperidone mechanism of action infographics. Image: re-cognition.center
Primary Pharmacodynamic Effects
The therapeutic efficacy of risperidone stems from its sophisticated interaction with multiple neurotransmitter systems in the central nervous system:
1. Dopaminergic System Modulation
Risperidone exhibits potent antagonism at dopamine D₂ receptors, particularly in the mesolimbic pathway. This D₂ receptor blockade correlates strongly with its antipsychotic efficacy. Unlike first-generation antipsychotics, risperidone demonstrates rapid dissociation kinetics from D₂ receptors—characterized as “hit and run” binding—which may contribute to its reduced extrapyramidal symptom profile. The drug achieves approximately 70-80% D₂ receptor occupancy at therapeutic doses, falling within the optimal therapeutic window.
2. Serotonergic System Interaction
A defining characteristic of risperidone is its high-affinity antagonism at serotonin 5-HT₂A receptors. The 5-HT₂A/D₂ affinity ratio significantly exceeds that of traditional antipsychotics, theoretically contributing to:
- Enhanced antipsychotic efficacy for negative symptoms
- Reduced extrapyramidal side effects through modulation of striatal dopamine release
- Improved cognitive symptom profiles
3. Additional Receptor Interactions
- α₁-adrenergic receptors: Moderate antagonism contributing to orthostatic hypotension
- α₂-adrenergic receptors: Weak antagonism
- Histamine H₁ receptors: Potent antagonism responsible for sedative effects and weight gain
- Muscarinic acetylcholine receptors: Minimal affinity, explaining reduced anticholinergic effects compared to older agents
Pharmacokinetic Considerations
| Parameter | Specification |
|---|---|
| Bioavailability | 70% (oral), unaffected by food |
| Protein Binding | 89% (primarily albumin and α₁-acid glycoprotein) |
| Metabolism | Hepatic via CYP2D6 (major) and CYP3A4 (minor) |
| Active Metabolite | 9-hydroxyrisperidone (paliperidone) |
| Half-life (parent compound) | 3-20 hours (extensive metabolizers: ~3h; poor metabolizers: ~20h) |
| Half-life (active metabolite) | 21-30 hours |
| Time to Steady State | 4-5 days |
| Peak Plasma Concentration | 1-2 hours (oral); 3 weeks (long-acting injection) |
| Elimination | Renal (70%) and fecal (14%) |
Metabolic Pathway Nuances
The CYP2D6 polymorphism significantly influences risperidone pharmacokinetics. Poor metabolizers (approximately 6-10% of Caucasians, lower in other ethnicities) demonstrate:
- 4-5 fold higher parent drug concentrations
- Lower 9-hydroxyrisperidone levels
- Potential need for dose reduction
- Increased risk of adverse effects at standard doses
What Is Risperidone Used For?
Schizophrenia Spectrum Disorders
Risperidone demonstrates efficacy across all symptom domains of schizophrenia:
- Positive symptoms: Hallucinations, delusions, thought disorder
- Negative symptoms: Affective flattening, avolition, alogia, asociality
- Cognitive symptoms: Working memory, executive function, attention deficits
- Affective symptoms: Depression and anxiety commonly comorbid with schizophrenia
Clinical trials demonstrate symptom reduction beginning within 1-2 weeks, with optimal therapeutic effects emerging after 4-6 weeks of consistent administration.
Bipolar I Disorder
- Acute manic or mixed episodes: Monotherapy or adjunctive therapy with lithium or valproate
- Maintenance treatment: Prevention of mood episode recurrence
- Pediatric approval: Treatment of manic or mixed episodes in children and adolescents aged 10-17 years
Irritability Associated with Autistic Disorder
Specifically approved for:
- Severe temper tantrums
- Self-injurious behavior
- Aggression toward others
- Rapid mood changes
- Pediatric patients aged 5-16 years
Off-Label Applications
| Condition | Evidence Level | Notes |
|---|---|---|
| Treatment-resistant depression (adjunctive) | Moderate | Augmentation of antidepressants |
| Obsessive-compulsive disorder | Limited | Second-line after failed SSRIs |
| Tourette syndrome | Moderate | Tic reduction |
| Post-traumatic stress disorder | Limited | Primarily for hyperarousal symptoms |
| Behavioral disturbances in dementia | Controversial | Black box warning regarding mortality |
| Personality disorders | Limited | Borderline personality, cluster B features |
| Substance-induced psychosis | Moderate | Short-term management |
Risperidone Dosage and Administration
Oral Dosage Guidelines
| Indication | Starting Dose | Titration | Therapeutic Range | Maximum Dose |
|---|---|---|---|---|
| Schizophrenia (adults) | 2 mg/day in 1-2 divided doses | Increase 1-2 mg/day at 24-hour intervals | 4-8 mg/day | 16 mg/day |
| Schizophrenia (adolescents 13-17) | 0.5 mg/day | Increase 0.5-1 mg/day at ≥3 day intervals | 1-6 mg/day | 6 mg/day |
| Bipolar mania (adults) | 2-3 mg/day as monotherapy; 1-2 mg/day as adjunct | Increase 1 mg/day | 1-6 mg/day | 6 mg/day |
| Bipolar mania (children 10-17) | 0.5 mg/day | Increase 0.5 mg/day at ≥3 day intervals | 1-2.5 mg/day | 2.5 mg/day |
| Autistic irritability (children 5-16) | 0.25 mg/day (<20kg) or 0.5 mg/day (≥20kg) | Increase at ≥2 week intervals | 0.5-3 mg/day | 3 mg/day (>45kg: 6 mg/day) |
| Elderly/dementia | 0.25 mg twice daily | Slow titration essential | 0.5-2 mg/day | 2 mg/day |
Long-Acting Injectable (LAI) Formulation
Risperidone Consta®
- Initial dosing: Establish oral tolerability first; 25 mg intramuscular injection every 2 weeks
- Dose conversion: Generally, oral daily dose × 2 = biweekly LAI dose (e.g., 4 mg oral ≈ 25 mg LAI; 6 mg oral ≈ 37.5 mg LAI; 8 mg oral ≈ 50 mg LAI)
- Administration: Deep intramuscular injection into deltoid (initiation) or gluteal (maintenance) muscle
- Supplementation: Continue oral risperidone (or alternative antipsychotic) for 3 weeks following first injection
- Dose adjustments: Increments of 12.5 mg at 4-week intervals; maximum 50 mg every 2 weeks
Risperidone Perseris® (extended-release subcutaneous injection)
Risperidone Perseris is used as follows:
- Monthly administration
- Different pharmacokinetic profile requiring specific conversion protocols
Special Populations Dosing
Hepatic Impairment
- Mild to moderate: Initiate at 0.5 mg twice daily; slower titration
- Severe: Use contraindicated or extreme caution with 0.25 mg daily initial dosing
Renal Impairment
- Clearance reduced by 60% in severe renal impairment
- Initiate at 0.5 mg twice daily
- Titrate more conservatively
Pediatric Considerations
- Weight-based dosing often employed
- Monitor growth velocity, sexual maturation, and cognitive development
- Regular assessment of metabolic parameters essential
Risperidone Side Effects
Common Adverse Effects (≥10% incidence)
| System | Adverse Effect | Frequency | Management Strategy |
|---|---|---|---|
| Central Nervous | Extrapyramidal symptoms (EPS) | Dose-dependent | Dose reduction, anticholinergic agents, switch to lower EPS agent |
| Akathisia | 10-20% | Beta-blockers, benzodiazepines, dose reduction | |
| Somnolence | 10-25% | Bedtime dosing, gradual titration | |
| Headache | 10-15% | Analgesics, usually transient | |
| Insomnia | 5-15% | Morning dosing, sleep hygiene | |
| Metabolic | Weight gain | 15-25% | Dietary counseling, exercise programs, metabolic monitoring |
| Hyperprolactinemia | 30-60% | Dose reduction, switching agents if symptomatic | |
| Cardiovascular | Orthostatic hypotension | 10-15% | Gradual titration, hydration, compression stockings |
| Tachycardia | 5-10% | Monitor, usually benign | |
| Endocrine | Amenorrhea/Galactorrhea | 10-30% (females) | Prolactin monitoring, endocrinology referral if persistent |
| Sexual dysfunction | 10-25% | Dose reduction, phosphodiesterase inhibitors, switching | |
| Gynecomastia | 2-10% (males) | Reassurance, surgical intervention if severe | |
| Gastrointestinal | Constipation | 10-15% | Fiber, hydration, stool softeners |
| Nausea | 5-10% | Usually transient, antiemetics if needed | |
| Dyspepsia | 5-10% | Antacids, PPIs | |
| Other | Rhinitis | 5-10% | Antihistamines, nasal steroids |
Serious Adverse Effects of Risperidone
Neuroleptic Malignant Syndrome (NMS)
- Rare (0.01-0.02%) but potentially fatal
- Characterized by hyperthermia, muscle rigidity, autonomic instability, altered consciousness, elevated creatine kinase
- Immediate discontinuation, supportive care, dantrolene or bromocriptine if severe
Tardive Dyskinesia (TD)
- Cumulative incidence: 4-5% annually (lower than first-generation agents)
- Risk increases with duration of exposure and age
- Potentially irreversible; early detection through AIMS examination crucial
Metabolic Syndrome
- Weight gain: Average 2-3 kg in first year
- Dyslipidemia: Elevated triglycerides, decreased HDL
- Hyperglycemia/Diabetes mellitus: Risk increased 1.5-2 fold
- Monitoring protocol: Baseline and quarterly weight, waist circumference; fasting glucose and lipids at baseline, 12 weeks, then annually
Cardiovascular Concerns
- QTc prolongation: Minimal at therapeutic doses; caution with other QTc-prolonging agents
- Cerebrovascular events: Increased risk in elderly with dementia (black box warning)
- Venous thromboembolism: Rare association, mechanism unclear
Hematologic
- Neutropenia: Rare; monitor if concomitant myelosuppressive agents
- Agranulocytosis: Extremely rare compared to clozapine
Endocrine Disruption
- Hyperprolactinemia: Dose-dependent; can lead to bone density loss with chronic elevation, increased breast cancer risk theoretical concern
- Diabetes insipidus: Rare central DI presentation
Special Populations Risks
Elderly with Dementia-Related Psychosis
- Black Box Warning: Increased mortality risk (1.6-1.7 fold) primarily due to cardiovascular or infectious events
- Increased cerebrovascular adverse events (stroke, TIA)
- Use only when behavioral interventions fail and patient poses danger to self/others
Pediatric Patients
- Long-term effects on growth, sexual maturation, and cognitive development not fully established
- Monitoring of height, weight, Tanner staging essential
- Risk of hyperprolactinemia-related bone density effects with chronic use
Pregnancy and Lactation
- Pregnancy Category C: Animal studies show adverse effects; limited human data
- Third-trimester exposure: Risk of EPS or withdrawal symptoms in neonates (agitation, tremor, hypotonia, feeding disorder)
- Lactation: Excreted in breast milk; concentration ratio milk: plasma approximately 0.4; weigh risks vs. benefits
Risperidone and Drug Interactions
Pharmacokinetic Interactions
| Interaction Type | Specific Agents | Clinical Effect | Management |
|---|---|---|---|
| CYP2D6 Inhibition | Fluoxetine, paroxetine, bupropion, quinidine | ↑ Risperidone levels, ↓ 9-hydroxyrisperidone | Reduce risperidone dose 50% or switch antidepressant |
| CYP3A4 Induction | Carbamazepine, phenytoin, phenobarbital, rifampin | ↓ Risperidone levels 40-50% | Increase risperidone dose; monitor levels |
| CYP3A4 Inhibition | Ketoconazole, itraconazole, erythromycin, clarithromycin | ↑ Risperidone levels | Reduce risperidone dose; monitor for adverse effects |
| Competitive Inhibition | Valproic acid | Variable effects on risperidone metabolism | Monitor clinical response |
| Protein Binding Displacement | Warfarin (theoretical) | Minimal clinical significance | Standard INR monitoring |
Pharmacodynamic Interactions
| Interaction Class | Specific Concerns | Clinical Consequence | Recommendation |
|---|---|---|---|
| CNS Depressants | Benzodiazepines, opioids, alcohol | Additive sedation, respiratory depression | Caution with combination; dose reduction |
| Antihypertensives | All classes | Additive hypotension | Blood pressure monitoring, dose adjustment |
| QTc Prolonging Agents | Class IA/III antiarrhythmics, macrolides, antipsychotics | Increased torsades de pointes risk | ECG monitoring, avoid if possible |
| Dopamine Agonists | Levodopa, dopamine agonists for Parkinson’s | Antagonism of therapeutic effects | Avoid in Parkinson’s disease psychosis if possible; consider pimavanserin |
| Anticholinergics | Benztropine, trihexyphenidyl | Additive cognitive impairment, constipation | Minimize anticholinergic burden |
| Serotonergic Agents | SSRIs, SNRIs, triptans, tramadol | Serotonin syndrome (rare) | Monitor for hyperthermia, clonus, autonomic instability |
Food and Herbal Interactions
- Grapefruit juice: CYP3A4 inhibition potential; avoid large quantities
- St. John’s Wort: CYP3A4 induction; reduce efficacy
- Caffeine: Minimal interaction
- Alcohol: Additive CNS depression; avoid or minimize
Contraindications and Precautions
Absolute Contraindications
- Hypersensitivity to risperidone, paliperidone, or formulation components
- Severe CNS depression or comatose states
Relative Contraindications / Major Precautions
| Condition | Concern | Action Required |
|---|---|---|
| Dementia-related psychosis (elderly) | Increased mortality, cerebrovascular risk | Avoid if possible; if necessary, informed consent, limited duration |
| Parkinson’s disease/Lewy body dementia | Severe sensitivity to EPS, worsening parkinsonism | Contraindicated; consider quetiapine or clozapine |
| History of NMS | Recurrence risk | Extreme caution, slow titration, monitoring |
| Seizure disorders | Lowered seizure threshold | Monitor seizure frequency, adjust anticonvulsants |
| Cardiovascular disease | Orthostatic hypotension, QTc effects | ECG baseline, orthostatic vital signs |
| Diabetes mellitus | Worsening glycemic control | Enhanced glucose monitoring |
| Hyperprolactinemic disorders | Exacerbation (prolactinomas) | Baseline prolactin, endocrinology consultation |
| Bone marrow suppression | Additive myelosuppressive risk | Regular CBC monitoring |
| Suicide risk | Overdose lethality (relatively safer than TCAs, but still concerning) | Limited quantities, supervision |
| Phenylketonuria | Orally disintegrating tablets contain phenylalanine | Use conventional tablets |
Monitoring Parameters
Baseline Assessment (Pre-Treatment)
| Parameter | Rationale |
|---|---|
| Comprehensive psychiatric evaluation | Confirm diagnosis, establish symptom severity baseline |
| Medical history and physical examination | Identify contraindications, comorbidities |
| Weight, height, BMI | Baseline for metabolic monitoring |
| Waist circumference | Central adiposity marker |
| Fasting plasma glucose or HbA1c | Diabetes screening |
| Fasting lipid profile | Dyslipidemia screening |
| Blood pressure (supine and standing) | Orthostatic hypotension risk |
| ECG | QTc baseline, cardiac risk stratification |
| Prolactin level (especially females) | Baseline for hyperprolactinemia monitoring |
| CBC with differential | Baseline hematologic status |
| Liver function tests | Hepatic metabolism consideration |
| Renal function tests | Renal elimination consideration |
| Pregnancy test (females of childbearing potential) | Pregnancy safety |
| AIMS or Dyskinesia rating scale | Baseline movement disorder assessment |
Ongoing Monitoring Schedule
| Timeframe | Parameters |
|---|---|
| Weeks 1-4 | Weight weekly; vital signs each visit; EPS assessment; sedation level |
| Weeks 6-12 | Weight; fasting glucose and lipids; prolactin if symptomatic; AIMS |
| Quarterly | Weight, BMI, waist circumference; blood pressure; metabolic panel if abnormal |
| Annually | Fasting glucose and lipids; prolactin (females, or if symptoms); AIMS; CBC; LFTs |
| As indicated | ECG if cardiac symptoms; additional assessments based on clinical presentation |
Is Risperidone Overdose Possible?
Toxicity Profile
Risperidone demonstrates relatively high therapeutic index compared to many psychotropic agents. Fatalities are rare in monotherapy overdose.
Dose-Related Symptoms:
- <100 mg: Mild to moderate sedation, tachycardia, hypotension, EPS
- 100-300 mg: Significant CNS depression, respiratory compromise, prolonged QTc
- >300 mg: Severe toxicity potential, seizures, arrhythmias, coma
Clinical Presentation of Overdose
| System | Manifestations |
|---|---|
| CNS | Drowsiness, sedation, ataxia, tremor, dystonia, seizures (rare), coma |
| Cardiovascular | Tachycardia, hypotension (orthostatic and supine), QTc prolongation, torsades de pointes (rare) |
| Respiratory | Respiratory depression (rare with monotherapy) |
| Other | Hyperprolactinemia symptoms, neuroleptic malignant syndrome (rare) |
Management Protocol
- Immediate Measures
- Airway protection; intubation if GCS <8
- Cardiac monitoring (continuous telemetry)
- IV access; fluid resuscitation for hypotension
- Activated charcoal if within 1-2 hours and airway protected
- Specific Interventions
- Hypotension: Trendelenburg positioning, IV fluids; avoid epinephrine (ineffective with α-blockade); use norepinephrine or phenylephrine
- Seizures: Benzodiazepines (lorazepam, diazepam)
- Arrhythmias: Magnesium for torsades; overdrive pacing if refractory
- EPS: Anticholinergics if severe dystonia
- Enhanced Elimination
- Hemodialysis/hemoperfusion: NOT effective (high protein binding, large volume of distribution)
- Forced diuresis: Not recommended
- Supportive Care
- Continuous monitoring for 24-48 hours due to long half-life of active metabolite
- Psychiatric evaluation once medically cleared
Clinical Pharmacology in Special Populations
Pediatric Patients
Pharmacokinetic Differences:
- Higher weight-adjusted clearance in children
- Shorter half-life compared to adults
- Rapid hepatic metabolism
Efficacy Considerations:
- FDA-approved for autism (5-16 years) and bipolar mania/schizophrenia (adolescents)
- Response rates comparable to adults in approved indications
- Long-term safety data limited beyond 2 years
Safety Monitoring:
- Growth velocity (height, weight) every 3-6 months
- Sexual maturation (Tanner staging)
- Cognitive and academic performance
- Metabolic parameters (more frequent than adults due to developmental vulnerability)
Geriatric Patients
Pharmacokinetic Changes:
- Reduced hepatic clearance (20-40% decrease)
- Reduced renal clearance
- Increased body fat/water ratio
- Decreased albumin (affects free drug concentration)
Clinical Implications:
- Start low (0.25-0.5 mg/day), go slow
- Target doses typically 0.5-2 mg/day
- Increased sensitivity to:
- Orthostatic hypotension (fall risk)
- EPS (even at low doses)
- Sedation (cognitive impairment, delirium)
- Anticholinergic effects (urinary retention, constipation, confusion)
Pregnancy and Postpartum
Teratogenicity Data:
- Limited controlled studies; no definitive teratogenic signal
- Animal studies: Increased pup mortality, developmental delays
- Human data: Slight increase in congenital malformations in some databases, but confounded by maternal illness and polypharmacy
Third Trimester Considerations:
- Risk of neonatal adaptation syndrome (NAS): Tremor, agitation, abnormal muscle tone, feeding difficulties, respiratory distress
- Monitor neonates for 48-72 hours if third-trimester exposure
Lactation:
- Relative infant dose (RID) approximately 2.3-4.7% of maternal weight-adjusted dose
- Monitor infants for sedation, feeding difficulties, developmental milestones
- Consider alternative feeding if high maternal doses (>6 mg/day)
Risperidone vs. Other Antipsychotics
| Feature | Risperidone | Olanzapine | Quetiapine | Aripiprazole | Haloperidol |
|---|---|---|---|---|---|
| EPS Risk | Moderate (dose-dependent) | Low | Very low | Very low | High |
| Metabolic Effects | Moderate | High | Moderate | Minimal | Minimal |
| Sedation | Moderate | High | High | Minimal | Moderate |
| Prolactin Elevation | High | Low | Low | Minimal | High |
| QTc Effects | Minimal | Minimal | Moderate | Minimal | Moderate-High |
| Anticholinergic Effects | Minimal | Low | Low | Minimal | Moderate |
| Weight Gain | Moderate (2-3 kg/year) | High (5-10 kg/year) | Moderate (2-4 kg/year) | Minimal | Minimal |
| Generic Availability | Yes | Yes | Yes | Yes | Yes |
| LAI Formulation | Yes | Yes (olanzapine pamoate) | No | Yes | Yes (decanoate) |
| Cost | Low (generic) | Low (generic) | Low (generic) | Moderate | Low |
Position in Treatment Algorithms
Schizophrenia:
- First-line: Along with other SGAs; preferred when compliance concern suggests LAI need
- Consider when: Prominent positive symptoms, need for LAI, patient preference for daily oral medication with established efficacy
Bipolar Disorder:
- First-line: For manic episodes, especially with psychotic features
- Maintenance: Effective but metabolic monitoring essential; consider if lithium/valproate insufficient or intolerable
Autism Spectrum Disorder:
- First-line: For severe irritability when behavioral interventions insufficient
- Only FDA-approved pharmacotherapy for this indication in pediatric population
Frequently Asked Questions About Risperidone
How long does it take risperidone to work?
Some effects may begin within hours (sedation), while antipsychotic effects typically develop over 1-3 weeks. Full benefits may take 4-6 weeks.
Can I stop taking risperidone suddenly?
No. Abrupt discontinuation can lead to withdrawal symptoms or relapse. Always taper under medical supervision.
Will risperidone change my personality?
Risperidone treats symptoms of mental illness rather than changing personality. By reducing symptoms like paranoia or aggression, others may perceive changes in behavior.
Is risperidone addictive?
Risperidone isn’t considered addictive in the traditional sense. It doesn’t produce cravings or drug-seeking behavior, but the body may develop physiological dependence, requiring gradual tapering.
How does risperidone compare to other antipsychotics like Abilify?
Each medication has a unique side effect profile and efficacy pattern. Abilify typically causes less weight gain and metabolic issues but may be more activating than risperidone.
What is the lowest dose of risperidone?
0.25 mg/day. This is the typical starting dose for:
- Elderly patients with dementia-related psychosis
- Pediatric patients with autistic disorder weighing less than 20 kg
- Patients with severe hepatic or renal impairment
What is the maximum dose of risperidone?
16 mg/day. This is the absolute maximum approved dose for adults with schizophrenia.
Clinically recommended maximums:
- Schizophrenia: 4–8 mg/day (higher doses show minimal additional benefit)
- Bipolar disorder: 6 mg/day
- Pediatric patients: 3–6 mg/day (depending on indication and age)
- Long-acting injection: 50 mg every 2 weeks
Is risperidone an antipsychotic?
Yes. Risperidone is a second-generation (atypical) antipsychotic. It is FDA-approved for:
- Schizophrenia (all symptom domains)
- Bipolar I disorder (acute manic/mixed episodes and maintenance)
- Irritability associated with autistic disorder
What is the best time to take risperidone?
Flexible timing, but typically at bedtime due to its sedative effects.
Key considerations:
- Can be taken once or twice daily, with or without food
- Bedtime dosing is often preferred to minimize daytime drowsiness
- If insomnia occurs, switching to morning dosing may help
- Consistency is more important than specific timing
Can risperidone cause weight gain?
Yes. Weight gain is one of the most common metabolic side effects.
Details:
- Incidence: 15–25% of patients experience clinically significant weight gain
- Magnitude: Average of 2–3 kg (4.4–6.6 lbs) in the first year
- Mechanism: Histamine H₁ receptor antagonism and other metabolic effects
- Risk factors: Higher doses, longer duration, younger age, and lower baseline BMI
Can risperidone cause hallucinations?
No. Risperidone is used to treat hallucinations, not cause them.
Important notes:
- Paradoxical reactions: Extremely rare cases of worsening psychosis or new symptoms may occur, usually due to rapid dose changes or individual sensitivity.
- Withdrawal hallucinations: Abrupt discontinuation can cause rebound psychosis with hallucinations—always taper gradually.
If hallucinations occur or worsen while on risperidone, it typically indicates:
- Inadequate dosing
- Treatment-resistant symptoms
- Need for medication review or switch
Can risperidone cause anxiety?
Yes, though it’s more complex:
- Akathisia (inner restlessness/urge to move) occurs in 10–20% of patients and is frequently misinterpreted as anxiety.
- Activation syndrome: Early in treatment, some patients experience increased anxiety, agitation, or insomnia.
- Withdrawal anxiety: Missing doses or abrupt discontinuation can cause rebound anxiety.
Can risperidone cause depression?
Yes, though it’s primarily used to treat depressive symptoms in bipolar disorder and schizophrenia.
Potential mechanisms for depressive effects:
- Neuroleptic-induced deficit syndrome: Emotional blunting, apathy, or anhedonia from excessive D₂ blockade (usually at higher doses).
- Secondary negative symptoms: Can mimic or worsen depression.
- Prolactin elevation: Chronic hyperprolactinemia can contribute to mood changes and anhedonia.
Quick Reference Summary Table
| Question | Answer |
|---|---|
| Lowest dose | 0.25 mg/day |
| Maximum dose | 16 mg/day (adult schizophrenia); 6 mg/day (bipolar) |
| Is it an antipsychotic? | Yes — second-generation (atypical) |
| Best time to take | Bedtime (due to sedation) or morning if insomnia occurs |
| Weight gain? | Yes — 15-25% incidence; ~2-3 kg average |
| Cause hallucinations? | No — treats them; rare paradoxical reactions possible |
| Cause anxiety? | Yes — often via akathisia; 10-20% incidence |
| Cause depression? | Possible — via emotional blunting or high-dose effects; also treats depression in bipolar disorder |
References and Further Reading
This encyclopedia entry is synthesized from primary literature, FDA prescribing information, clinical practice guidelines (APA, CANMAT, NICE), and pharmacology texts. For specific clinical decisions, consult current prescribing information and evidence-based guidelines.
Key Guidelines:
1. American Psychiatric Association (APA) Practice Guideline for the Treatment of Patients with Schizophrenia
- Full PDF: psychiatryonline.org/doi/pdf/10.1176/appi.books.9780890424841
- APA Psychiatry Online: psychiatryonline.org/doi/book/10.1176/appi.books.9780890424841
2. CANMAT/ISBD Guidelines for the Management of Patients with Bipolar Disorder
- Full Text (PMC):
- Psychopharmacology Institute Summary (with PDF): psychopharmacologyinstitute.com/section/canmat-isbd-guidelines-for-bipolar-depression-2274-4404/
3. NICE Guidelines for Psychosis and Schizophrenia in Children and Young People
- Official NICE Guideline (HTML): nice.org.uk/guidance/cg155
- PubMed Summary: pubmed.ncbi.nlm.nih.gov/26065063/
Sources & References
- Janssen Pharmaceuticals (2023) Risperdal® (risperidone) tablets/orally disintegrating tablets/oral solution: prescribing information. Titusville, NJ: Janssen. Available at: https://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/RISPERDAL-pi.pdf
- Leucht, S. et al. (2013) ‘Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis’, The Lancet, 382(9896), pp. 951–962. Available at: https://pubmed.ncbi.nlm.nih.gov/23810019/
- Citrome, L. (2009) ‘Risperidone: a review of its use in the management of irritability associated with autistic disorder in children and adolescents’, CNS Drugs, 23(4), pp. 307–318. Available at: https://pubmed.ncbi.nlm.nih.gov/19320575/
- Correll, C.U. (2008) ‘Antipsychotic use in children and adolescents: minimizing adverse effects to maximize outcomes’, Journal of the American Academy of Child & Adolescent Psychiatry, 47(1), pp. 9–20. Available at: https://pubmed.ncbi.nlm.nih.gov/18174828/
- Haddad, P.M. and Sharma, S.G. (2007) ‘Adverse effects of atypical antipsychotics: differential risk and clinical implications’, CNS Drugs, 21(11), pp. 911–936. Available at: https://pubmed.ncbi.nlm.nih.gov/17927296/