
ADHD: Neurology or Poor Parenting?
We explore why ADHD is not tantrums but neurobiology, which signs should alert parents already in preschool age, and which methods truly help a child learn, communicate, and cope with demands.
ADHD is one of the most discussed and simultaneously most misunderstood conditions of childhood development.
Despite decades of research, persistent myths continue to exist around it. Some parents believe it’s simply “being spoiled” or “lack of strictness,” others think the diagnosis is given too often, and still others believe ADHD is incurable and turns a child into “problematic.”
The reason for disputes is that many manifestations of ADHD resemble ordinary behavior of active children:
- restlessness,
- curiosity,
- emotionality.
But in the case of ADHD, we’re not talking about momentary tantrums or character, but about a neurobiological peculiarity of brain function.
Modern medicine views ADHD as a disorder of nervous system development that has clear criteria and confirmed mechanisms.
An additional difficulty is that a child’s behavior depends on their environment. If the family doesn’t know what’s happening and reacts with punishments or criticism, symptoms become more noticeable. This creates a false impression that “poor parenting” is the root cause. However, research shows: parenting can strengthen or weaken manifestations, but does not cause ADHD.
Today it’s important for parents to understand: ADHD is a reality confirmed by science, and with competent help, such children can develop just as successfully as their peers.
Child Psychiatrist Marcus Evans: “Still, a significant portion of parents and even educators consider ADHD a consequence of parental inexperience or incorrect upbringing, and this is one of the reasons why the topic provokes so many emotional disputes. At the foundation of ADHD lie neurobiological peculiarities in the development of the frontal parts of the brain, but it’s difficult for people to accept that a child’s behavior can be a consequence of physiological processes rather than character. Often families are embarrassed to turn to specialists, fearing they’ll be accused of ‘the wrong approach.’
In my practice, I encounter cases where children go for years with the label ‘lazy’ or ‘ill-mannered,’ although they had obvious signs of ADHD. The earlier parents receive scientifically confirmed information, the lower the child’s risk of encountering low self-esteem and school difficulties. It’s very important to abandon accusations and move toward cooperation with specialists. This isn’t a ‘fashionable diagnosis’ but a real condition that can be corrected with a competent approach. The more a family knows about the nature of ADHD, the easier it is to select help strategies that truly work.”
What is ADHD: Symptoms, Mechanisms, Brain Peculiarities
ADHD (Attention Deficit Hyperactivity Disorder) is a neurodevelopmental condition in which a child has impaired ability to maintain attention, control impulses, and regulate activity level. At its foundation lie peculiarities in the functioning of the frontal lobes of the brain and neurotransmitters, primarily dopamine and norepinephrine.
Main components of ADHD:
- Attention deficit — the child is easily distracted, cannot concentrate on a task for long, “switches off” in the process.
- Impulsivity — acts without thinking, interrupts, reacts sharply, has difficulty controlling emotions.
- Hyperactivity — excessive mobility, constant need for movement, sensation of an “internal motor.”
Neurologist David Richardson: “The main peculiarity of children with ADHD is impaired regulation of attention and behavior, connected to peculiarities in the functioning of the prefrontal cortex. Many parents are surprised why a child can spend hours building with construction sets but isn’t capable of listening to a short instruction. The thing is that with ADHD, attention works on the principle of ‘interest — activation’ rather than ‘must — activation.’
The neurotransmitter system, especially dopamine, functions differently, which makes it harder for the brain to maintain concentration on tasks that don’t bring immediate reward. This isn’t laziness and not an absence of will, but physiology. It’s important to understand that these children possess normal or even high intelligence. They often think outside the box, show strong imagination, can quickly solve tasks where creativity is required. But to unlock this potential, they need a structured environment and support from adults.”
At the same time, the brains of children with ADHD work differently:
- activity of areas responsible for self-control and planning is reduced;
- transmission of signals regulating attention and behavior is disrupted;
- the brain becomes exhausted faster under mental load.
It’s important to understand that a child with ADHD doesn’t choose their behavior. They cannot “just pull themselves together,” “calm down,” or “stop getting distracted,” as adults sometimes demand.
These skills are formed with the help of special strategies, support, and adapted approaches.
First Signs That Are Noticeable in Preschool Age
Often parents see peculiarities in their child as early as 3-5 years old but don’t connect them with ADHD, considering them normal or “temperament.”
In reality, many symptoms are noticeable quite early.
What might alert parents:
- It’s very difficult for the child to sit still even for a short time: they fidget, jump up, run without apparent reason.
- Often abandons started activities and switches to something new, not finishing a game or task.
- It seems the child doesn’t hear addressed speech — not because they’re ignoring it, but because they “switch off” from the situation.
- Play is chaotic: many actions, little sequence, difficulty following rules.
- The child speaks quickly, interrupts, blurts out answers, doesn’t wait their turn.
- Frequent emotional outbursts: the child can quickly become overexcited or upset “out of nowhere.”
- There are difficulties with self-care and routine tasks — for example, they might start getting dressed and a minute later forget what they should be doing.

It can be a real challenge for parents to manage ADHD in preschool age. Image: re-cognition.center
At the same time, such children often display high intelligence, lively imagination, capacity for original thinking. But their potential can be “lost” due to difficulties with attention and self-regulation.
The earlier parents notice signs and turn to specialists, the easier it is for the child to learn to manage their behavior and develop strong sides.
How ADHD Manifests in School
Image: re-cognition.center
Starting school is a moment when a child’s peculiarities become especially noticeable. Academic demands increase, the need for prolonged concentration, self-control, and following rules appears. For a child with ADHD, this can be a serious test.
Most often in the school environment, ADHD manifests like this:
- Difficulties with attention in lessons. The child “zones out,” gets distracted by any movement or sound, cannot follow the teacher’s instruction from beginning to end.
- Mistakes due to rushing. They may know the material but perform tasks hurriedly, skipping letters, steps, or details.
- Problems with organization. Notebooks get lost, homework is forgotten, school supplies end up in different places.
- Impulsivity in behavior. The child blurts out answers, interrupts, may get up from their seat without waiting for permission.
- Difficulties with observing boundaries. Peers may complain that the child “butts into games,” violates rules, or reacts too vigorously.
- Overload and fatigue. By evening, the child is often exhausted, which can lead to bursts of irritability and tears.
Most school difficulties in children with ADHD aren’t about intellect but about peculiarities in performing tasks that require prolonged attention control.
ADHD Is Not Poor Parenting: What Actually Influences Symptom Development
Despite widespread myths, ADHD doesn’t arise from “parental softness,” “inconsistency,” or “permissiveness.”
This condition has a neurobiological foundation, and its symptoms are formed under the influence of:
- Genetics. In 70-80% of children with ADHD, there’s a relative with similar peculiarities.
- Peculiarities of nervous system development. Important is the functioning of frontal lobes that regulate attention, self-control, planning.
- Disrupted neurotransmitter transmission. Dopamine and norepinephrine in such children function differently, which affects the ability to maintain attention and manage impulses.
- Pregnancy and early age factors. Hypoxia, prematurity, complicated births can increase risk.
At the same time, parenting style is not a cause of ADHD but can influence the severity of symptoms:
- an emotionally calm, structured environment reduces impulsivity and hyperactivity;
- constant criticism, punishments, unpredictability intensify difficulties.
Therefore, blaming parents or the child is incorrect and harmful. What’s important is understanding, being informed, and providing support.
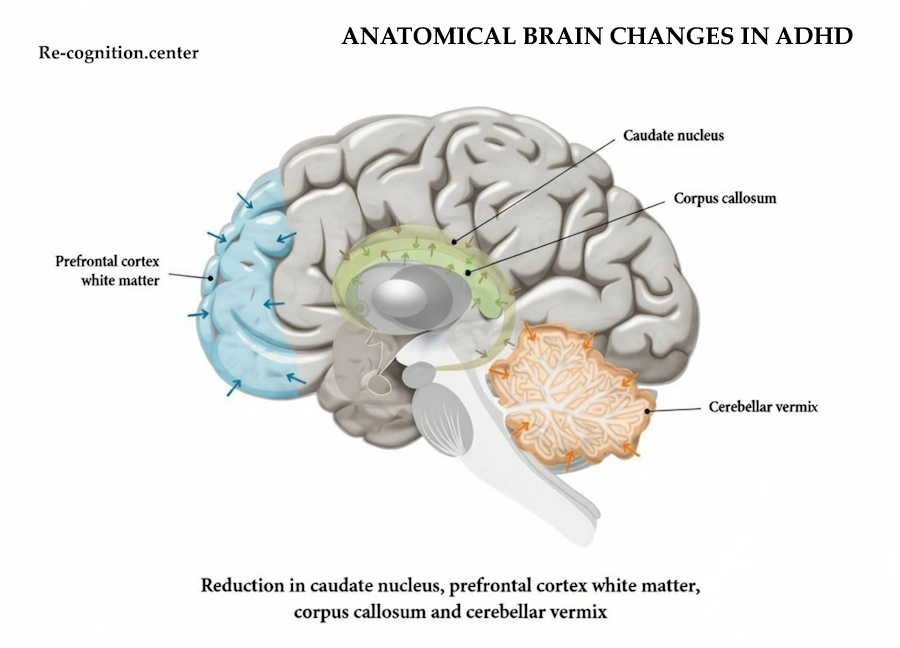
Anatomical Brain Changes in ADHD: Highlighting reductions in key brain regions like the caudate nucleus, prefrontal cortex white matter, corpus callosum, and cerebellar vermis. Image: re-cognition.center
This image is a colorful diagram of the brain from the side, showing specific parts that are often smaller or reduced in people with ADHD. The blue area is the white matter in the prefrontal cortex (involved in planning and focus), the green spots are the caudate nucleus and corpus callosum (helping with movement, attention, and connecting brain halves), and the orange part is the cerebellar vermis (aids in coordination and behavior regulation). It’s a visual way to show how ADHD can involve actual differences in brain structure, not just behavior.
Diagnosis: Who and How Diagnoses ADHD
An ADHD diagnosis isn’t made “by eye” or after one visit. It’s a comprehensive assessment including observations, conversations, and special scales.
Diagnosis is conducted by:
- child neurologist;
- child psychiatrist;
- clinical psychologist (conducts testing and questionnaires).
Usually diagnosis includes:
- Medical history collection. The specialist studies manifestations from early childhood.
- Behavior comparison in different environments. ADHD is characterized by presence of symptoms in at least two spheres: at home, at daycare, or school.
- Psychological testing. Standardized methodologies are used (for example, Conners, Vanderbilt).
- Child observation. The specialist assesses impulsivity, peculiarities of motor activity, concentration.
- Exclusion of other causes. Hearing or vision disorders, anxiety disorders, consequences of stress.
A diagnosis is made only after comprehensive assessment, not based on one symptom.
What Helps Children with ADHD: Scientifically Proven Correction Methods
The modern approach views ADHD as a condition that can be effectively corrected. Combined methods that consider developmental peculiarities and family needs help many children. Scientifically proven strategies include:
1. Behavioral therapy. Parents are taught specific techniques:
- clear rules and predictability;
- consistent reward system;
- development of self-regulation skills;
- working with impulsive reactions.
2. Parent training programs. They help:
- build daily structure;
- reduce the number of conflicts;
- learn to give instructions that the child can realistically fulfill.
3. Educational support. At school, these help:
- task adaptation;
- reduction of written work volume;
- visual prompts;
- possibility of movement breaks.
4. Medication therapy. Prescribed only by a psychiatrist and not always necessary. It can:
- improve ability to concentrate;
- reduce hyperactivity;
- increase productivity in lessons.
5. Attention and executive function training. These are games and methods that develop:
- planning;
- information retention in memory;
- impulse control;
- thinking flexibility.
6. Daily routine. Sleep, nutrition, physical activity directly affect ADHD manifestations.
It’s very important not to overload the child — their nervous system becomes exhausted faster, so activity changes and small breaks are mandatory. Physical activity is a powerful helper: it improves concentration and reduces hyperactivity. Family parent training programs give results no worse than medication if symptoms are moderately expressed. The main thing is to stop perceiving ADHD as a behavior problem and work with it as a developmental peculiarity that can be successfully influenced.”
ADHD is a peculiarity of brain function that requires understanding, competent diagnosis, and support.
Children with ADHD grow up curious, creative, bright, and very lively — if there are adults nearby who help them cope with difficulties, build understandable rules, and notice even small successes. Modern approaches allow significantly easing the life of the child and family, reducing symptom manifestations, and improving adaptation at school and in everyday life.
Sources & References
- American Psychiatric Association (2022) Diagnostic and Statistical Manual of Mental Disorders, 5th ed., Text Revision (DSM-5-TR). Washington, DC: American Psychiatric Association.
- World Health Organization (2022) International Classification of Diseases, 11th Revision (ICD-11). Geneva: World Health Organization.
- Faraone, S.V. et al. (2021) ‘The World Federation of ADHD International Consensus Statement: 208 Evidence-Based Conclusions about the Disorder’, Neuroscience & Biobehavioral Reviews, 128, pp. 789–818.
- Cortese, S. (2020) ‘Current Concepts in the Treatment of Attention Deficit Hyperactivity Disorder’, New England Journal of Medicine, 383, pp. 1050–1056.
- Shaw, P. et al. (2012) ‘Neurodevelopmental Trajectories of the Human Cerebral Cortex in Attention-Deficit/Hyperactivity Disorder’, Biological Psychiatry, 72(4), pp. 327–334.
- Volkow, N.D. and Swanson, J.M. (2013) ‘Clinical Implications of the Neuroscience of ADHD’, Annual Review of Clinical Psychology, 9, pp. 9.1–9.23.
- Rubia, K. (2018) ‘Neuroimaging of Attention Deficit Hyperactivity Disorder: Current Status and Future Directions’, European Child & Adolescent Psychiatry, 27(3), pp. 265–284.
- Sonuga-Barke, E.J.S. et al. (2011) ‘Preschool Attention-Deficit/Hyperactivity Disorder: Diagnostic Validity, Clinical Implications, and Treatment Options’, Neuropsychiatric Disease and Treatment, 7, pp. 567–581.
- Egger, H.L. and Angold, A. (2006) ‘Common Emotional and Behavioral Disorders in Preschool Children: Presentation, Nosology, and Epidemiology’, Journal of Child Psychology and Psychiatry, 47(3–4), pp. 313–337.
- Chronis-Tuscano, A. et al. (2013) ‘Parent Training for Preschool ADHD: The Role of Parental Depression and Stress’, Journal of Abnormal Child Psychology, 41(7), pp. 1073–1084.
- Johnston, C. and Mash, E.J. (2001) ‘Families of Children with ADHD: Review and Recommendations for Future Research’, Clinical Child and Family Psychology Review, 4(3), pp. 183–207.
- National Institute for Health and Care Excellence (NICE) (2019) Attention Deficit Hyperactivity Disorder: Diagnosis and Management (NG87). London: National Institute for Health and Care Excellence.
- Pelham, W.E. et al. (2022) ‘Behavioral and Combined Treatments for ADHD: Evidence Base and Practice Recommendations’, Clinical Psychology Review, 91, 102112.
- Evans, S.W., Owens, J.S. and Bunford, N. (2014) ‘Evidence-Based Psychosocial Treatments for Children and Adolescents with ADHD’, Journal of Clinical Child & Adolescent Psychology, 43(4), pp. 527–551.
- Centers for Disease Control and Prevention (CDC) (2024) ‘What Is ADHD?’, CDC. Available at: https://www.cdc.gov/adhd/index.html
- National Institute of Mental Health (NIMH) (2024) ‘Attention-Deficit/Hyperactivity Disorder’, NIMH. Available at: https://www.nimh.nih.gov/health/topics/attention-deficit-hyperactivity-disorder
Join the Conversation
Your email address will not be published.