Frontal Lobe Dementia: What It Is, What to Expect, and How to Cope
When someone you love starts acting differently — making strange decisions, losing their filter, or slowly forgetting who they are — it can be terrifying and confusing. If a doctor has mentioned the words “frontal lobe dementia,” you are probably looking for real answers right now. This article is written for you. We will walk through everything you need to know about this condition: what it is, how it starts, how it is diagnosed, and what lies ahead — in plain, honest language backed by trusted medical sources.
What Is Frontal Lobe Dementia?
Frontal lobe dementia is an umbrella term for a group of brain disorders caused by progressive damage to the frontal and temporal lobes of the brain. These are the regions that govern your personality, behavior, decision-making, language, and social awareness. Unlike Alzheimer’s disease, which primarily attacks memory first, frontal lobe dementia typically strikes personality and behavior first — which is why it is often missed or misdiagnosed in its early stages.
The medical community most commonly uses the term frontotemporal dementia (FTD) or frontotemporal lobar degeneration (FTLD) to describe this group of conditions. The National Institute of Neurological Disorders and Stroke (NINDS) recognizes it as one of the most common causes of early-onset dementia — meaning dementia that begins before age 65.
Frontotemporal dementia is not a single disease. It is a family of related syndromes, all rooted in the degeneration of the brain’s frontal and temporal lobes. What makes it so challenging — for patients, families, and doctors alike — is that it can look very different from one person to the next.
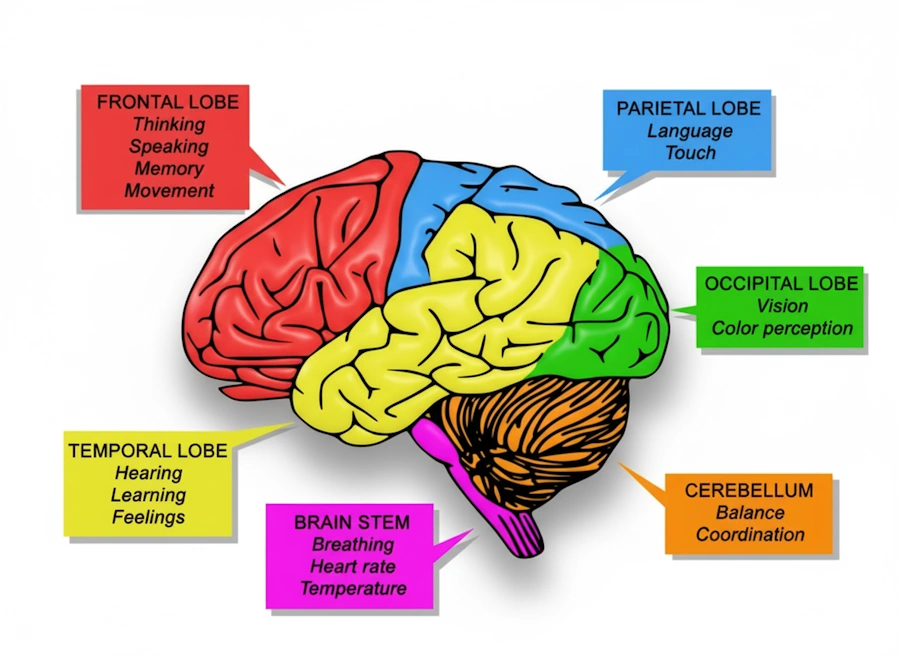
Illustration of brain lobes to visualize which lobe is answering for what bodily and cognitive function. Image: re-cognition.center
Types of Frontotemporal Dementia
Frontotemporal dementia is classified into several distinct syndromes based on which part of the brain is most affected and which symptoms appear first. Understanding the type can help make sense of what you or your loved one is experiencing.
| Type | Primary Area Affected | Hallmark Symptoms | Approximate Proportion of FTD Cases |
|---|---|---|---|
| Behavioral Variant FTD (bvFTD) | Frontal lobes | Personality changes, impulsivity, apathy, loss of empathy, socially inappropriate behavior | ~50–60% |
| Semantic Dementia (SD) | Left temporal lobe | Loss of word meaning, difficulty recognizing objects and faces, fluent but empty speech | ~20% |
| Nonfluent/Agrammatic Primary Progressive Aphasia (nfvPPA) | Left frontal/insular region | Slow, effortful speech, grammatical errors, difficulty forming sentences | ~20% |
| FTD with Motor Neuron Disease (FTD-MND) | Frontal lobes + motor neurons | Behavioral symptoms combined with muscle weakness and ALS-like features | ~10–15% |
| Progressive Supranuclear Palsy (PSP) | Frontal lobes + brainstem | Balance problems, eye movement difficulties, stiffness, personality changes | Overlapping syndrome |
| Corticobasal Syndrome (CBS) | Frontal and parietal lobes | Limb rigidity, apraxia, alien limb phenomenon, cognitive decline | Overlapping syndrome |
How Common Is Frontal Lobe Dementia?
Frontotemporal dementia affects an estimated 50,000 to 60,000 people in the United States at any given time, according to the Association for Frontotemporal Degeneration (AFTD). It is considered the second most common cause of dementia in people under 65, after Alzheimer’s disease. It affects men and women roughly equally, and most people are diagnosed between the ages of 45 and 65 — though it can occur in people as young as their 20s or as old as their 80s.
Because it often strikes during working years, FTD has a devastating impact not only on the individual but on entire families — affecting employment, finances, and caregiving responsibilities in ways that Alzheimer’s, which more commonly affects older adults, does not always create.
What Causes Frontal Lobe Dementia?
At the cellular level, frontal lobe dementia is caused by the abnormal accumulation of certain proteins in the brain’s neurons. These protein deposits disrupt normal cell function and eventually cause neurons to die. The specific protein involved varies by subtype and plays a role in predicting disease progression and genetic risk.
Key Protein Pathologies in FTD
| Protein | Associated FTD Subtype(s) | Notes |
|---|---|---|
| TDP-43 | bvFTD, SD, FTD-MND | Most common pathology; also seen in ALS |
| Tau | nfvPPA, PSP, CBS, some bvFTD | Also linked to Alzheimer’s disease and CTE |
| FUS (Fused in Sarcoma) | Rare FTD cases, often younger onset | Less common; associated with atypical presentations |
Genetic Causes
Genetics plays a significant role in frontal lobe dementia. Approximately 30 to 40 percent of people with FTD have a family history of the condition, and 10 to 15 percent have a clearly identified genetic mutation. The three most common genetic causes are:
- C9orf72 repeat expansion — the most common known genetic cause of FTD, also linked to ALS
- GRN (progranulin) gene mutations — cause TDP-43 pathology; may respond to certain treatments in the future
- MAPT (microtubule-associated protein tau) mutations — directly affect tau protein and cause tau-related FTD
If FTD runs in your family, speaking with a genetic counselor can provide important information about your own risk. Genetic testing is available and may be appropriate in some situations — your neurologist can guide this conversation.
Sporadic Cases
In the majority of cases — about 60 to 70 percent — there is no clear family history, and no identifiable genetic mutation is found. These are called sporadic cases. The cause in these individuals remains an active area of research, with environmental factors, aging processes, and complex gene-environment interactions under study.
Early Signs and Symptoms

One of the most difficult aspects of frontal lobe dementia is that its early symptoms are often mistaken for something else entirely. Depression, midlife crisis, personality conflicts, psychiatric illness — all of these have been wrongly blamed before the real diagnosis was made. Knowing what to watch for can make a real difference in how quickly someone gets the help they need.
Behavioral and Personality Changes (Most Common in bvFTD)
- Loss of empathy — the person seems indifferent to the feelings of others, including those they love
- Social disinhibition — making rude, inappropriate, or embarrassing comments in public without awareness
- Impulsive behavior — acting without thinking, making poor financial decisions, shoplifting, overeating
- Apathy — complete loss of motivation and interest, often mistaken for depression
- Compulsive or repetitive behaviors — repeating words, phrases, or routines; collecting objects; tapping
- Changes in food preferences — strong cravings for sweets or a sudden change in diet
- Neglecting personal hygiene — no longer caring about bathing, grooming, or dressing appropriately
- Loss of insight — the person does not recognize that their behavior has changed
Language and Speech Changes
- Difficulty finding words during conversation
- Speaking less often or becoming nearly mute
- Using the wrong words, inventing new ones, or struggling to understand language
- Slow, labored, or grammatically unusual speech
- Difficulty reading or writing even when speaking is still possible
What Is Often Preserved (Especially Early On)
Unlike Alzheimer’s disease, frontal lobe dementia often leaves certain abilities intact for a surprisingly long time. This can add to the confusion — the person may still remember recent events clearly, navigate familiar environments, and perform basic self-care tasks, while simultaneously making alarming decisions or acting in ways completely out of character.
| Ability | Typically Preserved in Early FTD | Typically Affected in Early Alzheimer’s |
|---|---|---|
| Recent memory | Often preserved | Often impaired early |
| Spatial orientation | Often preserved | Often impaired |
| Personality and behavior | Severely affected | More gradually affected |
| Language | Affected in some subtypes | Usually preserved early |
| Social judgment | Severely affected | More gradually affected |
| Insight into illness | Usually absent | Often partially present early |
How Is Frontal Lobe Dementia Diagnosed?
There is no single test that diagnoses FTD. A diagnosis is built over time from multiple sources of information — clinical history, cognitive testing, brain imaging, and sometimes genetic testing. Because FTD mimics so many other conditions, the diagnostic process can take months to years. This is not a failure of medicine; it is the nature of the disease.
Step-by-Step Diagnostic Process
1. Medical History and Clinical Interview
A neurologist will conduct a thorough history — ideally with both the patient and a close family member or caregiver present. The family member’s account is often more revealing than the patient’s, because insight is frequently impaired. The doctor will ask about when changes began, how they progressed, and whether there is a family history of dementia or psychiatric illness.
2. Neuropsychological Testing
Detailed cognitive testing evaluates specific brain functions including attention, executive function, language, memory, and social cognition. Tools used may include:
- Mini-Mental State Examination (MMSE)
- Montreal Cognitive Assessment (MoCA)
- Frontal Assessment Battery (FAB)
- Cambridge Behavioural Inventory (CBI)
3. Brain Imaging
Structural and functional imaging studies are central to FTD diagnosis.
| Imaging Type | What It Shows | Use in FTD Diagnosis |
|---|---|---|
| MRI (Magnetic Resonance Imaging) | Brain structure, atrophy patterns | Shows shrinkage of frontal and/or temporal lobes; rules out stroke, tumor |
| FDG-PET Scan | Brain glucose metabolism | Shows reduced activity in frontal/temporal regions even before visible atrophy |
| SPECT Scan | Blood flow patterns | Detects hypoperfusion in frontal lobes; useful when MRI is inconclusive |
| Amyloid PET | Amyloid plaque deposition | Used to rule out Alzheimer’s disease (FTD is amyloid-negative) |
4. Blood Tests and Lumbar Puncture
Blood tests rule out other reversible causes of cognitive change, such as thyroid dysfunction, vitamin B12 deficiency, or liver disease. Cerebrospinal fluid (CSF) analysis via lumbar puncture may show protein markers that help differentiate FTD from Alzheimer’s disease. Emerging blood biomarkers, including neurofilament light chain (NfL) and phosphorylated tau ratios, are being studied as diagnostic tools.
5. Genetic Testing
When there is a family history of FTD, ALS, or early-onset dementia, genetic testing for known mutations (C9orf72, GRN, MAPT) may be recommended. Results have implications not only for the patient but for biological relatives and should be accompanied by genetic counseling.
Diagnostic Criteria
Current clinical diagnosis of behavioral variant FTD relies on the International Consensus Criteria (Rascovsky et al., 2011), which require at least three of the following six features to be present:
- Disinhibition — socially inappropriate behavior
- Apathy or inertia
- Loss of sympathy or empathy
- Perseverative, stereotyped, or compulsive/ritualistic behavior
- Hyperorality or dietary changes
- Neuropsychological profile consistent with frontal or temporal dysfunction
Conditions That Can Be Mistaken for Frontal Lobe Dementia
Because behavioral and personality changes are its most prominent early features, FTD is regularly misdiagnosed. Studies suggest that the average time from symptom onset to correct diagnosis is 3.6 years. Knowing the most common misdiagnoses can help you advocate for the right workup.
| Condition Often Confused with FTD | Why the Confusion Occurs |
|---|---|
| Major Depression | Apathy, withdrawal, and loss of motivation overlap significantly |
| Bipolar Disorder | Impulsivity and poor judgment can resemble a manic episode |
| Schizophrenia | Personality disorganization and social withdrawal look similar |
| Alzheimer’s Disease | Both are progressive dementias; early FTD may have normal memory |
| Personality Disorder | Behavioral changes are attributed to longstanding character traits |
| Substance Abuse | Disinhibition and poor judgment are attributed to alcohol or drugs |
| Midlife Crisis | Changes in priorities and relationships are dismissed as psychological |
If you believe something neurological is happening and a psychiatric explanation does not feel right, trust your instincts and request a referral to a neurologist with expertise in cognitive disorders. An FTD specialist center — many affiliated with major university hospitals — can be an invaluable resource.
Stages of Frontal Lobe Dementia
FTD progresses through recognizable stages, though the rate varies significantly from person to person. Some individuals decline rapidly over two to three years; others live with the disease for ten years or more. The average duration from symptom onset to death ranges from 6 to 11 years, depending on the subtype and individual factors.
Early Stage
Subtle personality shifts that are easy to dismiss. The person may seem irritable, rude, or apathetic. Social withdrawal or, conversely, socially inappropriate behavior. Language difficulties begin in language-variant FTD. Judgment and decision-making become problematic. Memory and orientation are usually intact.
Middle Stage
Behavioral changes become impossible to ignore. The person may be unable to work or manage finances. Language deteriorates — in behavioral variant FTD, speech may become very sparse. Compulsive behaviors intensify. Physical symptoms such as balance problems or tremors may emerge in PSP or CBS variants. Caregiving needs increase substantially.
Late Stage
The person becomes heavily dependent on caregivers for all activities of daily living. Swallowing difficulties (dysphagia) become a serious concern. Mobility is often severely impaired. Communication may be reduced to single words or absent. Weight loss and susceptibility to infection increase. In those with FTD-MND, respiratory muscles may be affected.
Treatment: What Can Be Done
There is currently no disease-modifying treatment that can stop or reverse frontal lobe dementia. However, there is a great deal that medicine and supportive care can offer. The goal of treatment is to manage symptoms, maintain quality of life for as long as possible, and support both the person with FTD and their family.
Medications Used in FTD Management
There are no drugs are specifically approved by the U.S. Food and Drug Administration (FDA) for FTD. However, certain medications are used off-label to manage specific symptoms.
| Symptom Target | Medication Class | Examples | Important Notes |
|---|---|---|---|
| Behavioral symptoms, impulsivity, disinhibition | SSRIs (Selective Serotonin Reuptake Inhibitors) | Sertraline, Fluvoxamine, Paroxetine | Often first-line; can reduce compulsive behaviors and irritability |
| Agitation, aggression | Atypical antipsychotics | Quetiapine, Olanzapine | Used cautiously; increased risk of adverse effects in dementia |
| Depression, apathy | SNRIs or SSRIs | Venlafaxine, Sertraline | May improve motivation; limited evidence specifically for FTD |
| Motor symptoms (in PSP/CBS) | Dopaminergic agents | Levodopa/Carbidopa | Modest benefit in some patients; response is limited |
| Pseudobulbar affect (involuntary laughing/crying) | Combination agent | Dextromethorphan/Quinidine (Nuedexta) | FDA-approved for pseudobulbar affect; may help in some FTD cases |
Important: Medications used for Alzheimer’s disease — particularly cholinesterase inhibitors such as donepezil (Aricept) — are generally not recommended in FTD and may worsen behavior. Always work with a neurologist experienced in FTD when making medication decisions.
Non-Pharmacological Therapies
Non-drug approaches form the backbone of FTD care and can meaningfully improve daily life.
- Speech-language therapy — helps maintain communication as long as possible; introduces augmentative communication tools when speech declines
- Occupational therapy — adapts the home environment, recommends adaptive equipment, and helps maintain independence in daily tasks
- Physical therapy — addresses balance, mobility, fall prevention, and movement difficulties in motor-variant syndromes
- Behavioral management strategies — structured routines, environmental modifications, and redirection techniques that reduce agitation and compulsive behaviors
- Music therapy and sensory stimulation — can engage and calm individuals who respond less to verbal communication
- Nutritional support — dietary management for hyperorality and overeating in early stages; pureed diets and thickened liquids when swallowing becomes unsafe
Emerging and Investigational Treatments
Research into FTD is accelerating. Several promising areas are under active investigation:
- Progranulin-targeting therapies — for patients with GRN mutations, treatments that restore progranulin levels (including gene therapy approaches) are in clinical trials
- Antisense oligonucleotides (ASOs) — designed to target C9orf72 repeat expansions; early human trials are underway
- Tau-targeted therapies — including tau aggregation inhibitors and immunotherapy approaches for tau-related FTD variants
- TDP-43 research — understanding how to prevent pathological TDP-43 accumulation remains an active area
If you or your loved one has a genetic form of FTD, asking your neurologist about clinical trial eligibility is worth doing. The ALLFTD consortium and the Advancing Research and Treatment for Frontotemporal Lobar Degeneration (ARTFL) network maintain registries and conduct trials specifically in FTD populations.
Living with Frontal Lobe Dementia: A Guide for Families
Caring for someone with FTD is one of the most emotionally complex experiences a family can face. The behavioral changes — the loss of empathy, the impulsive actions, the seeming indifference — can make it feel like the person you love has already left, even when they are still physically present. This grief has a name: ambiguous loss. It is real, it is profound, and you are not alone in feeling it.
Practical Strategies for Daily Caregiving
- Establish routine. People with FTD often find predictable schedules calming. Consistent meal times, activities, and bedtimes reduce anxiety and minimize disruptive behavior.
- Simplify the environment. Remove clutter, lock up medications and chemicals, and reduce household hazards before they become problems.
- Address driving early. Impaired judgment makes driving dangerous well before the person recognizes it themselves. Work with the medical team to address this proactively, ideally with the help of a neuropsychologist’s driving assessment.
- Protect finances. Impulsive spending, susceptibility to scams, and poor financial judgment are common and can be financially catastrophic. Consider a durable power of attorney and working with an elder law attorney early in the disease.
- Do not argue with the behavior. Trying to reason with someone whose reasoning centers are damaged rarely works and often escalates. Redirection, distraction, and calm responses are far more effective.
- Communicate with the whole team. Keep primary care physicians, specialists, therapists, and social workers informed. FTD management works best as a team effort.
Safety Concerns Specific to FTD
| Risk Area | Why It Matters in FTD | Recommended Action |
|---|---|---|
| Driving | Poor judgment and impulsivity before motor impairment appears | Formal driving evaluation; consider early cessation |
| Financial management | Impulsive spending, susceptibility to fraud | Power of attorney; remove access to large funds |
| Social/legal issues | Disinhibited behavior may lead to legal trouble | Obtain medical documentation; consult an attorney if needed |
| Falls | Motor variants cause balance problems; apathy reduces activity | Home safety assessment; physical therapy |
| Nutrition | Hyperorality and food-seeking behavior; later dysphagia | Monitor food access; swallowing evaluation when needed |
| Medication management | Person may take too much or refuse medication | Caregiver-controlled dispensing; blister packs |
Caregiver Self-Care
Caregiver burnout in FTD is real and well-documented. The behavioral nature of the disease makes caregiving uniquely stressful compared to other dementias. You are not a better caregiver for refusing to ask for help. In fact, sustaining yourself is one of the most important things you can do for the person in your care.
- Connect with an FTD-specific caregiver support group — either locally or online through the Association for Frontotemporal Degeneration (AFTD)
- Accept respite care and home health services; do not wait until you reach a crisis point
- Work with a therapist or counselor who understands caregiver grief and ambiguous loss
- Talk to your own doctor about your physical and mental health
- Plan ahead — legal, financial, and placement decisions are easier to make before you are exhausted
Prognosis: What to Expect Over Time
Every FTD journey is different, and prognosis depends significantly on the subtype, the underlying protein pathology, and individual factors. That said, understanding the general trajectory can help families plan thoughtfully.
| FTD Subtype | Typical Survival from Symptom Onset | Notes |
|---|---|---|
| Behavioral Variant FTD (bvFTD) | 6–11 years | Wide variation; some genetic forms progress faster |
| Semantic Dementia (SD) | 8–12 years | Often longer course; language decline prominent |
| Nonfluent PPA (nfvPPA) | 7–10 years | Speech loss often precedes behavioral and functional decline |
| FTD-MND (with ALS features) | 2–3 years | Shortened by respiratory and swallowing complications |
| Progressive Supranuclear Palsy (PSP) | 5–7 years | Falls and aspiration pneumonia are common causes of death |
| Corticobasal Syndrome (CBS) | 6–8 years | Variable; motor and cognitive decline together |
The most common causes of death in FTD are aspiration pneumonia (often resulting from swallowing difficulties), respiratory complications, and general medical decline. Palliative care involvement — focused on comfort and quality of life — should ideally begin well before the very end stages.
Planning Ahead: Legal and Financial Considerations
One of the most loving things you can do when an FTD diagnosis is received is to begin legal and financial planning immediately — while the person still has the legal capacity to participate in decisions. This is not giving up. It is an act of care.
- Durable Power of Attorney (DPOA) — designates someone to handle financial decisions when the person can no longer do so
- Healthcare Proxy / Medical Power of Attorney — designates someone to make medical decisions
- Advance Directive / Living Will — documents the person’s wishes about life-sustaining treatment, hospitalization, and end-of-life care
- POLST (Physician Orders for Life-Sustaining Treatment) — a medical order that travels with the person and guides emergency responders
- Estate planning — wills, trusts, and beneficiary designations should be reviewed and updated
An elder law attorney can help navigate these documents. Social workers at FTD specialty centers are also valuable resources for connecting families with community services, financial assistance programs, and long-term care planning support.
Frequently Asked Questions
Is frontal lobe dementia the same as Alzheimer’s disease?
No. While both are progressive brain diseases, they are distinct conditions caused by different underlying processes in different areas of the brain. Alzheimer’s disease primarily involves amyloid plaques and tau tangles in regions governing memory, while frontal lobe dementia involves different protein accumulations in the frontal and temporal lobes. Their symptoms, progression, and management differ significantly.
Can frontal lobe dementia be prevented?
There are currently no proven methods to prevent FTD. Research is ongoing, but no lifestyle factor has been definitively identified as a cause or preventive measure the way cardiovascular risk factors have been linked to vascular dementia. In families with known genetic mutations, presymptomatic genetic testing and counseling are available, though no preventive interventions currently exist.
Is frontal lobe dementia hereditary?
It can be. Approximately 30 to 40 percent of people with FTD have a family history, and 10 to 15 percent carry an identifiable genetic mutation. If FTD runs in your family, genetic counseling is recommended before pursuing genetic testing, as the results carry significant implications.
Can someone with FTD live alone?
In very early stages, some individuals maintain independence with appropriate support and monitoring. However, the impaired judgment, impulsivity, and lack of insight that characterize FTD make independent living unsafe far sooner than memory impairment alone would. Safety assessments and honest conversations with the medical team are essential.
Will the person know what is happening to them?
One of the most painful features of FTD — particularly the behavioral variant — is that many individuals have very limited awareness of their own changes. This is not denial; it is a direct result of damage to the areas of the brain responsible for self-awareness. For family members, this lack of insight can feel like an additional loss. It also means that the person is often not suffering in the way they might if they had full awareness of their condition.
What is the difference between FTD and Pick’s disease?
Pick’s disease is an older term that was once used to describe what we now call frontotemporal dementia, specifically cases where abnormal protein accumulations called “Pick bodies” are found in the brain. Today, Pick’s disease is considered a pathological subtype within the broader FTD spectrum, not a completely separate condition.
Are there support groups for FTD?
Yes. The Association for Frontotemporal Degeneration (AFTD) is the leading organization in the United States dedicated specifically to FTD. They offer caregiver helplines, online support groups, a HelpLine staffed by trained professionals, educational resources, and connections to research programs. Their website at theaftd.org is an excellent starting point.
When to Seek a Specialist
If you are noticing changes in a loved one’s personality, behavior, or language — especially in someone under 65 — and something simply does not feel right, trust that feeling. Seeking evaluation from a behavioral neurologist or a memory disorders center is always the right call. A specialist in cognitive disorders or movement disorders (depending on the symptoms) will have the experience to conduct a thorough assessment and, if needed, refer you to an FTD center of excellence.
Early and accurate diagnosis matters. Not because there is a cure — not yet — but because the right diagnosis unlocks the right support, the right planning, and access to research that may one day make a difference for the next generation.
Key Takeaways
- Frontal lobe dementia (frontotemporal dementia) affects personality, behavior, and language — not primarily memory, especially early on
- It is one of the most common causes of dementia in people under 65
- Multiple subtypes exist, caused by abnormal accumulation of proteins (TDP-43, tau, or FUS) in the frontal and temporal lobes
- Genetic factors play a role in 30 to 40 percent of cases; three genes account for most familial cases
- Diagnosis requires clinical evaluation, cognitive testing, and brain imaging; no single test confirms FTD
- There is no approved disease-modifying treatment, but symptoms can be managed with medications, therapies, and behavioral strategies
- Survival from onset averages 6 to 11 years depending on the subtype
- Early legal and financial planning is one of the most important steps a family can take
- Caregivers need and deserve support — reaching out to organizations like the AFTD is a sign of strength, not weakness
Sources & References
- Rascovsky K, Hodges JR, Knopman D, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain. 2011;134(9):2456–2477. PMC4824317
- Gorno-Tempini ML, Hillis AE, Weintraub S, et al. Classification of primary progressive aphasia and its variants. Neurology. 2011;76(11):1006–1014. PMC4824317
- Bang J, Spina S, Miller BL. Frontotemporal dementia. Lancet. 2015;386(10004):1672–1682. PMC4824317
- Olney NT, Spina S, Miller BL. Frontotemporal dementia. Neurol Clin. 2017;35(2):339–374. PMC4824317
- Onyike CU, Diehl-Schmid J. The epidemiology of frontotemporal dementia. Int Rev Psychiatry. 2013;25(2):130–137. PMC3953732
- Perry DC, Whitwell JL, Boeve BF, et al. Clinical and imaging features of frontotemporal dementia. Neurol Clin. 2013;31(1):193–213. PMC4824317
- Woolley JD, Khan BK, Murthy NK, Miller BL, Rankin KP. The diagnostic challenge of psychiatric symptoms in neurodegenerative disease. J Clin Psychiatry. 2011;72(2):126–133. PubMed
- Mackenzie IRA, Neumann M, Bigio EH, et al. Nomenclature and nosology for neuropathologic subtypes of frontotemporal lobar degeneration. Acta Neuropathol. 2010;119(1):1–4. PMC4824317
- Sieben A, Van Langenhove T, Engelborghs S, et al. The genetics and neuropathology of frontotemporal lobar degeneration. Acta Neuropathol. 2012;124(3):353–372. PMC4824317
- Rohrer JD, Guerreiro R, Vandrovcova J, et al. The heritability and genetics of frontotemporal lobar degeneration. Neurology. 2009;73(18):1451–1456. PMC3953732
- DeJesus-Hernandez M, Mackenzie IRA, Boeve BF, et al. Expanded GGGGCC hexanucleotide repeat in C9ORF72 causes FTD and ALS. Neuron. 2011;72(2):245–256. PMC3953732
- Cruts M, Gijselinck I, Van der Zee J, et al. GRN mutations in FTD: pathogenic mechanisms and clinical implications. Acta Neuropathol. 2012;123(1):39–52. PMC3953732
- Hutton M, Lendon CL, Rizzu P, et al. Association of missense and 5′-splice-site mutations in tau with the inherited dementia FTDP-17. Nature. 1998;393(6686):702–705. PMC3953732
- Hu WT, McMillan CT, Grossman M. Biomarkers in frontotemporal lobar degeneration—progress and challenges. Neurotherapeutics. 2015;12(1):34–46. PMC4824317
- Whitwell JL. Neuroimaging in frontotemporal dementia. Int Rev Psychiatry. 2013;25(2):221–229. PMC4824317
- Meeter LH, Kaat LD, Rohrer JD, van Swieten JC. Imaging and fluid biomarkers in frontotemporal dementia. Nat Rev Neurol. 2017;13(7):406–419. PMC4824317
- O’Connor CM, Landin-Romero R, Clemson L, et al. Behavioral management in frontotemporal dementia: a systematic review of non-pharmacological interventions. Dement Geriatr Cogn Disord. 2017;44(5–6):318–331. PubMed
- Boxer AL, Boeve BF. Frontotemporal dementia treatment: current symptomatic therapies and implications of recent genetic, biochemical, and neuroimaging studies. Alzheimer Dis Assoc Disord. 2007;21(4):S79–S87. PubMed
- Mioshi E, Kipps CM, Dawson K, Mitchell J, Hodges JR. Activities of daily living in frontotemporal dementia and Alzheimer disease. Neurology. 2007;68(24):2077–2084. PubMed
- Onyike CU, et al. What is the life expectancy in frontotemporal lobar degeneration? (Life expectancy 7–13 years from onset; shorter with motor neuron disease). Neurology/related FTLD survival paper. PMC3953732