Pervasive Developmental Disorder – Not Otherwise Specified (PDD-NOS)
For nearly twenty years, Pervasive Developmental Disorder – Not Otherwise Specified (PDD-NOS) was the “catch-all” diagnosis of the psychiatric world. It was a confusing label, but a necessary one. It existed to capture the gray areas—the patients who were clearly on the autism spectrum but didn’t quite fit the rigid checklists for classical Autistic Disorder or Asperger’s Syndrome.
Even though the DSM-5 officially retired the label in 2013, merging it into the broader definition of Autism Spectrum Disorder (ASD), PDD-NOS is far from irrelevant. Understanding it is still vital because it provides context for the millions of adults diagnosed under the old system. It also helps us understand the subtle, “subthreshold” presentations of autism that clinicians still see every day [1].
This condition affects the very foundations of how we grow:
- how we connect socially
- how we communicate
- how flexible we are with our behavior.
But unlike the “textbook” version of autism, PDD-NOS was often fragmented. You might see a person with severe social struggles who speaks perfectly well, or someone with intense sensory pain but almost no repetitive behaviors.
The Evolution of the Diagnosis
To really get what PDD-NOS is, you have to look at the history of how we classify mental health. The idea of “pervasive developmental disorders” came from a simple need: clinicians needed a category for conditions that affected a child’s development across the board, not just in one specific skill.
Back in the DSM-IV era, PDD-NOS was one of five specific diagnoses. It sat alongside heavy hitters like Autistic Disorder, Asperger’s, Rett’s Disorder, and Childhood Disintegrative Disorder. In this landscape, PDD-NOS acted as the “subthreshold” category. Doctors used it when a patient had significant trouble with social interaction or showed repetitive behaviors, but didn’t tick enough boxes to qualify for the other specific disorders [2].
This led to a strange paradox. PDD-NOS became the most frequently used diagnosis in the autism world, yet it had the vaguest definition. It was an acknowledgement that neurodevelopment is a spectrum, even if the diagnostic manuals at the time were trying to force everything into neat little boxes.
The Shift to DSM-5
The arrival of the DSM-5 changed the game. The American Psychiatric Association recognized that the lines between Asperger’s, PDD-NOS, and classic Autism were often artificial; the diagnosis you got often depended more on which clinic you walked into than your actual biology.
To fix this, they consolidated everything into a single entity: Autism Spectrum Disorder (ASD). Today, most people who would have been called PDD-NOS are diagnosed with ASD, usually with a severity rating of Level 1 (requiring support) or Level 2 (requiring substantial support) [1]. However, the ICD-10—which is still the standard in many healthcare systems outside the US—still keeps the old code F84.9 for “Pervasive developmental disorder, unspecified.”

Fig 1. The Consolidation: How distinct categories in DSM-IV merged into the singular spectrum of DSM-5. Image: re-cognition.center
Clinical Presentation: The “Atypical” Profile
The defining characteristic of PDD-NOS was its heterogeneity. No two profiles looked exactly alike, which often complicated the diagnostic process. However, clinical observation reveals consistent patterns in social, communicative, and behavioral domains.
Social Interaction Nuances
While classical autism is often associated with a profound withdrawal, PDD-NOS presentations are frequently more nuanced. The impairment is qualitative.
- Eye Contact: It is rarely absent, but often ill-timed or inconsistent. An individual might hold gaze when listening but look away when speaking, or struggle to modulate eye contact during high-stress interactions [3].
- Peer Relationships: Young children might play alongside others (parallel play) rather than with them. Adolescents often possess a genuine desire for connection—unlike the aloofness sometimes seen in classical autism—but lack the “social intuitive” software to navigate complex teen dynamics.
- Reciprocity: Conversations may feel disjointed. The individual might struggle with the natural volley of dialogue, frequently pivoting back to their own interests without gauging the listener’s fatigue.
Communication Difficulties
Communication challenges in PDD-NOS are often less about the mechanics of speech and more about the use of speech (pragmatics).
- Language Development: Unlike Asperger’s (where no speech delay is permitted) and Autistic Disorder (where delay is common), PDD-NOS covered the middle ground. A child might have delayed milestones that eventually caught up [2].
- Literal Interpretation: The nuance of language—sarcasm, idioms, and metaphors—is frequently lost. A statement like “hop to it” might be confusing, as the individual processes the words at face value.
- Prosody: The rhythm of speech may sound “off”—perhaps too formal, monotonic, or pitched unusually high for the context.
Routine, Repetition, and Sensory Chaos
While the “classical” presentation of autism often involves a total, unyielding need for sameness, PDD-NOS can be more subtle. The rigidity is there—a change in plans might still ruin the day—but it is often less all-encompassing than in other parts of the spectrum.
The Role of Special Interests
Most of us have hobbies, but this goes deeper. We often see intense, focused passions. The difference lies in the intensity: these interests can consume so much mental space that there simply isn’t room for other activities. It isn’t just a preference for trains or maps; it is a fundamental need to engage with them to feel regulated.
Sensory Processing Issues
For many patients, the physical world is an assault. Things that neurotypical people ignore—the hum of a refrigerator, the scratch of a denim seam, or the flicker of overhead lights—can cause genuine physical pain. Conversely, “sensory seeking” behaviors also emerge. These are individuals who crave intense input, such as deep pressure, tight hugs, or constant motion, just to feel grounded in their bodies [4].
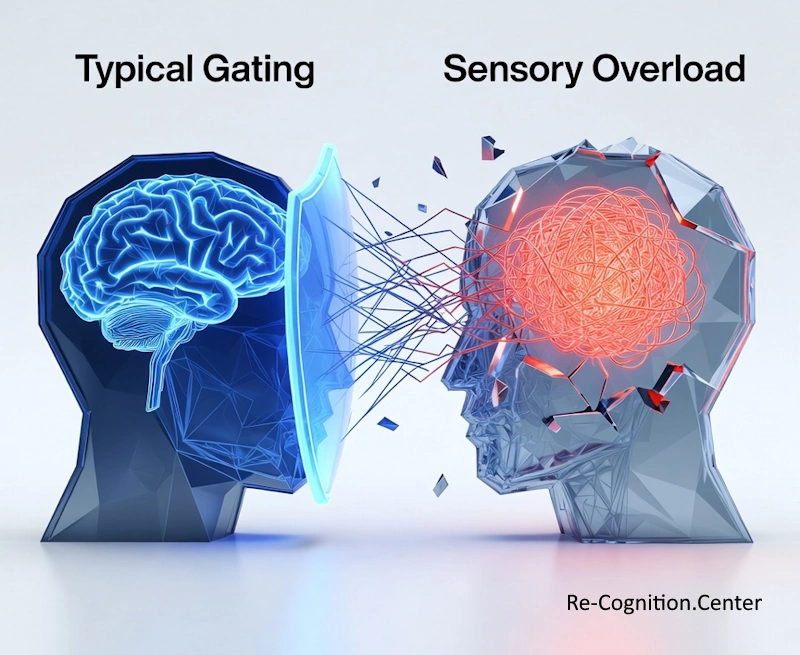
Illustration of a sensory overload in people with pervasive developmental disorder vs neurotypical people. Image: re-cognition.center
Etiology: The Biological Reality
We used to hunt for a single “autism gene,” but that search is largely over. Today, science views conditions like PDD-NOS not as a single error, but as a perfect storm. It is rarely just one cause; rather, it is a collision between built-in genetic risks and environmental factors.
The Genetic Landscape
The link between biology and family history is undeniable. Autism spectrum conditions are highly heritable; if one child has PDD-NOS, their siblings are statistically much more likely to have some form of neurodevelopmental difference. However, the genetics are messy. It usually breaks down into a combination of three mechanisms:
- De Novo Mutations: Sometimes, the genetics aren’t inherited at all. These are spontaneous errors—”glitches” in the sperm or egg that happen out of nowhere. They often hit the specific genes that control how synapses form in the brain [5].
- Copy Number Variations (CNVs): Imagine a book with missing or repeated pages. CNVs are deletions or duplications of DNA segments (such as the 16p11.2 region) that scramble the instructions for neural wiring.
- Polygenic Risk: This is the cumulative effect. It isn’t one “bad” gene, but rather thousands of tiny, common genetic variations. On their own, they do nothing, but when added together, they push a person over the threshold for the condition.
Neurobiology
Brain imaging suggests that this is a disorder of connectivity. The “under-connectivity theory” posits that while local brain networks (processing details) may be over-connected, long-range networks (integrating complex information) are under-connected. This explains why an individual might excel at memorizing facts (local processing) but struggle to interpret a social scenario (complex integration) [6].
Environmental Factors
While advanced paternal age and extreme prematurity are confirmed risk factors, it is clinically imperative to reinforce that vaccines do not cause PDD-NOS or autism. The initial 1998 paper suggesting such a link was based on fraudulent data and has been retracted; subsequent studies involving millions of children have found no causal association [7].
Assessment and Differential Diagnosis
Diagnosing PDD-NOS (now ASD) is a forensic process involving developmental history, direct observation, and standardized testing.
Clinicians rely on “gold standard” instruments like the Autism Diagnostic Observation Schedule (ADOS-2), which creates social presses to observe how the individual responds, and the Autism Diagnostic Interview-Revised (ADI-R), a deep-dive parent interview [3].
Differentiating PDD-NOS from other conditions is challenging.
- ADHD: Both involve social awkwardness and impulsivity. However, the child with ADHD usually understands social rules but acts too quickly to follow them; the child with PDD-NOS often does not intuitively understand the rule itself.
- Social Anxiety: An anxious child avoids interaction out of fear; a child with PDD-NOS avoids it (or engages awkwardly) due to a lack of skill or understanding.
- Social Communication Disorder: A newer DSM-5 diagnosis for those with pragmatic language issues without the repetitive behaviors or sensory issues of autism.
The Burden of Comorbidity
Rarely does PDD-NOS travel alone. Research suggests that up to 70% of individuals on the spectrum have at least one co-occurring condition [8].
- Mental Health: Anxiety disorders are rampant, affecting nearly half of this population. Depression is also common in adolescence as self-awareness of social differences grows.
- Physiological Issues: Sleep disorders (onset insomnia) and gastrointestinal distress (chronic constipation, reflux) are frequently reported, though the gut-brain connection remains under intense study.
- ADHD: Co-occurrence rates are estimated between 30-60%, creating a “double hit” on executive function and attention.
Intervention and Support

Lifelong Intervention: Therapeutic support often extends beyond childhood. Here, a clinician assists with fine motor coordination and task persistence—key components of occupational therapy that help individuals with ASD or PDD-NOS achieve greater independence in daily living. Image: re-cognition.center
Because the presentation of PDD-NOS is so variable, “cookie-cutter” therapies rarely work. Intervention must be tailored to the individual’s specific deficits.
Behavioral and Educational Support
- Applied Behavior Analysis (ABA) remains the most researched intervention, though modern approaches have shifted toward “naturalistic” implementations that prioritize the child’s motivation over rigid drilling.
- Social skills training is crucial for older children. This involves explicit instruction on “unwritten rules,” often using video modeling or “Social Stories” to decode complex interactions [9].
Therapeutic Modalities
- Occupational Therapy (OT): Essential for sensory integration and motor planning (praxis).
- Cognitive Behavioral Therapy (CBT): Highly effective for managing the anxiety and rigid thinking patterns often associated with the condition.
- Pharmacology: While no pill treats autism, medications like SSRIs (for anxiety) or stimulants (for ADHD) can significantly improve quality of life. Antipsychotics like risperidone are occasionally used for severe aggression or irritability, though the side effect profile requires caution.
Prognosis: Life After Diagnosis
The trajectory for someone with a PDD-NOS profile is heavily influenced by language ability and IQ. Unlike the grim outlooks of the past, we now know that many individuals go on to live independent, fulfilling lives.
Adult outcomes are variable. While some navigate higher education and employment successfully—often in fields that reward their specialized interests—others face “underemployment,” struggling with the soft skills required in the modern workplace. The transition to adulthood remains a critical cliff-edge where services often drop off.
Ultimately, the disappearance of the PDD-NOS label from the DSM-5 does not erase the lived experience of those who carried it. Whether viewed through a medical lens or the increasingly influential neurodiversity paradigm, the goal remains the same: not to “fix” the individual, but to provide the support and accommodation necessary for them to thrive on their own terms [10].
References
- American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5th ed. Arlington, VA: American Psychiatric Publishing.
- Volkmar, F.R. and McPartland, J.C. (2014). From Kanner to DSM-5: Autism as an Evolving Diagnostic Concept. Annual Review of Clinical Psychology, 10(1), pp.193–212.
- Lord, C., Rutter, M. and Le Couteur, A. (1994). Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24(5), pp.659–685.
- Marco, E.J., Hinkley, L.B.N., Hill, S.S. and Nagarajan, S.S. (2011). Sensory Processing in Autism: A Review of Neurophysiologic Findings. Pediatric Research, 69(5 Pt 2), pp.48R54R.
- Sanders, S.J. et al. (2015). Insights into Autism Spectrum Disorder Genomic Architecture and Biology from 71 Risk Loci. Neuron, 87(6), pp.1215–1233.
- Just, M.A., Cherkassky, V.L., Keller, T.A. and Minshew, N.J. (2004). Cortical activation and synchronization during sentence comprehension in high-functioning autism: evidence of underconnectivity. Brain, 127(8), pp.1811–1821.
- Taylor, L.E., Swerdfeger, A.L. and Eslick, G.D. (2014). Vaccines are not associated with autism: an evidence-based meta-analysis of case-control and cohort studies. Vaccine, 32(29), pp.3623–3629.
- Simonoff, E. et al. (2008). Psychiatric Disorders in Children With Autism Spectrum Disorders: Prevalence, Comorbidity, and Associated Factors in a Population-Derived Sample. Journal of the American Academy of Child & Adolescent Psychiatry, 47(8), pp.921–929.
- National Autism Center (2015). Findings and Conclusions: National Standards Project, Phase 2. Randolph, MA: National Autism Center.
- Howlin, P., Goode, S., Hutton, J. and Rutter, M. (2004). Adult outcome for children with autism. Journal of Child Psychology and Psychiatry, 45(2), pp.212–229.