Vascular Dementia: Causes, Symptoms, Stages, and Treatment
A dementia diagnosis can leave you with more questions than answers — and if blood flow to the brain is part of the conversation your doctor started, you may be searching for something that actually explains what that means for the person you care about, or for yourself. We will walk you through vascular dementia from the ground up: what is happening in the brain, why it happens, what to expect, and where to focus your energy.
What Is Vascular Dementia?
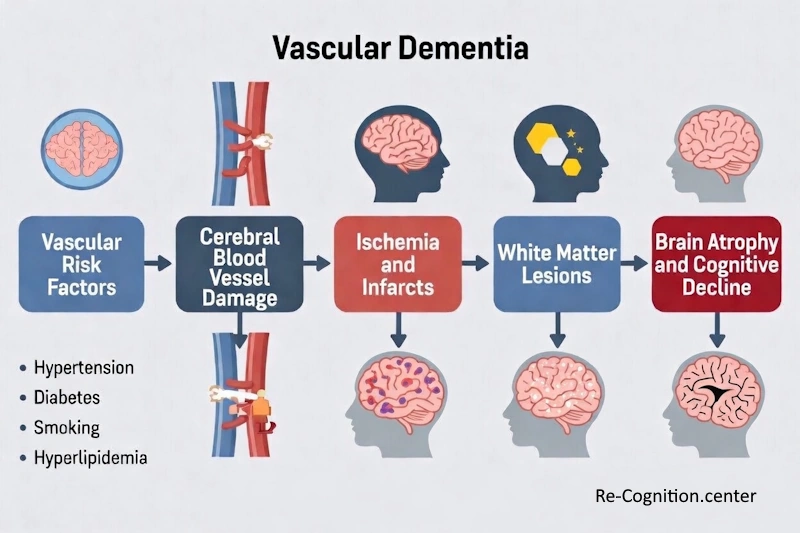
Vascular dementia is the second most common cause of dementia worldwide, ranking just behind Alzheimer’s disease. Rather than a single condition, it is a group of disorders that all share the same underlying problem: the brain is not receiving enough blood. When blood flow to brain tissue is reduced, interrupted, or cut off entirely — whether by a stroke, a series of small vessel injuries, or gradual arterial damage — brain cells are deprived of the oxygen and nutrients they need to survive. The damage that results can impair thinking, memory, reasoning, and behavior in ways that progressively affect daily life.
Your brain depends on a constant, rich supply of blood to function. That blood carries oxygen and nutrients to brain cells every second of every day. When blood flow is interrupted — even briefly — brain cells can become damaged or die. Over time, this damage adds up and begins to affect how the brain works, leading to the symptoms we recognize as vascular dementia.
Unlike Alzheimer’s disease, which involves the gradual buildup of abnormal proteins in the brain, vascular dementia is primarily a vascular (blood vessel) problem. This distinction matters because it means many of the risk factors for vascular dementia are the same risk factors as heart disease and stroke — and many of them are preventable or manageable.
How Common Is Vascular Dementia?
Vascular dementia accounts for approximately 10% to 20% of all dementia cases in the United States and Europe, according to the National Institute of Neurological Disorders and Stroke (NINDS). In older adults, it is often found alongside Alzheimer’s disease — a combination called mixed dementia — making it even more prevalent than pure case counts suggest.
The condition becomes significantly more common with age, and it affects men and women differently in some respects: men appear to develop vascular dementia at slightly higher rates, particularly following stroke, though women with dementia overall face longer disease courses.
Types of Vascular Dementia
Vascular dementia is not a single, uniform condition. It is an umbrella term that covers several distinct patterns of brain injury, each with its own characteristics.
Multi-Infarct Dementia (MID)
This condition results from multiple small strokes (infarcts) that occur over time. Each stroke causes a small area of brain damage, and the accumulated damage eventually leads to noticeable cognitive decline. Because symptoms worsen in a stepwise pattern — progressing after each stroke event rather than gradually — multi-infarct dementia can look different from Alzheimer’s disease, which tends to decline more smoothly.
Single Strategic Infarct Dementia
In some cases, a single stroke in a particularly important area of the brain — such as the thalamus, hippocampus, or angular gyrus — can cause dementia on its own. These “strategic” areas play such central roles in memory and cognition that damage to even a small portion produces significant and lasting effects.
Small Vessel Disease (Subcortical Vascular Dementia)
Small vessel disease involves damage to the tiny blood vessels deep inside the brain, in an area called the white matter. This type is often linked to long-standing high blood pressure and diabetes. It tends to progress more gradually than stroke-related dementia and is often detected on brain imaging as white matter changes or lesions. Binswanger’s disease is a specific subtype involving extensive white matter damage.
CADASIL
Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL) is a rare, inherited form of vascular dementia caused by mutations in the NOTCH3 gene. Unlike most vascular dementia, CADASIL can appear in people as young as their 30s or 40s. It is one of the most common hereditary causes of stroke and dementia in young adults.
Post-Stroke Dementia
When dementia develops within a few months following a major stroke, it is classified as post-stroke dementia. Studies show that up to one-third of people who survive a stroke may develop dementia within one year. The risk depends heavily on the location and severity of the stroke, as well as underlying brain health before the event.
Causes and Risk Factors
The underlying problem is always reduced or blocked blood flow to the brain — but what causes that reduced flow varies from person to person.
Primary Causes
| Cause | Description |
|---|---|
| Stroke (ischemic) | A blood clot blocks an artery supplying the brain, cutting off oxygen to brain tissue |
| Stroke (hemorrhagic) | A blood vessel ruptures, causing bleeding in or around the brain |
| Transient ischemic attacks (TIAs) | Brief, temporary blockages of blood flow (“mini-strokes”) that can cause cumulative damage |
| Cerebral small vessel disease | Narrowing or damage to small blood vessels deep in the brain, often linked to chronic high blood pressure |
| Atherosclerosis | Buildup of plaques inside artery walls that reduce blood flow over time |
Risk Factors
The risk factors for vascular dementia overlap heavily with those for heart disease and stroke — and that connection works in your favor. It means that the same steps proven to protect your heart also protect your brain, and many of those steps are well within reach through medical treatment and everyday choices.
| Risk Factor | Level of Influence | Modifiable? |
|---|---|---|
| High blood pressure (hypertension) | Very high | Yes |
| Type 2 diabetes | High | Partially |
| High cholesterol | High | Yes |
| Smoking | High | Yes |
| Atrial fibrillation (irregular heartbeat) | High | Partially |
| Obesity | Moderate to high | Yes |
| Physical inactivity | Moderate | Yes |
| History of stroke or TIA | Very high | Partially (can prevent recurrence) |
| Age (over 65) | Very high | No |
| Male sex | Moderate | No |
| Family history of stroke or vascular disease | Moderate | No |
| Sleep apnea | Moderate | Yes |
According to MedlinePlus, keeping blood pressure under control is considered one of the single most effective steps a person can take to reduce the risk of developing vascular dementia. High blood pressure over many years silently damages blood vessels throughout the body, including those in the brain — and the damage accumulates long before any symptoms appear.
Symptoms of Vascular Dementia
The symptoms of vascular dementia depend on which areas of the brain have been affected and to what degree. No two people experience vascular dementia in exactly the same way, which is one reason the condition can be difficult to recognize early on.
Vascular dementia is a slow cognitive decline with neurological symptoms. Image: re-cognition.center
That said, there are common patterns to watch for. Vascular dementia tends to affect executive function — the mental skills involved in planning, organizing, reasoning, and problem-solving — earlier and more prominently than memory, which is often the first thing people associate with dementia. Memory problems do occur, but they may not be the first or most obvious sign.
Cognitive Symptoms
- Difficulty with planning and organizing tasks
- Slower thinking and information processing
- Trouble concentrating or shifting attention
- Problems making decisions
- Difficulty with following some kind of sequence, for example – instructions
- Memory problems, particularly recalling recent events
- Confusion, especially in unfamiliar situations
- Language difficulties (finding words, following conversations)
Behavioral and Emotional Symptoms
- Depression, which is very common in vascular dementia
- Anxiety and restlessness
- Apathy and loss of motivation
- Emotional instability, including sudden crying or laughing (called pseudobulbar affect)
- Personality changes
- Social withdrawal
- Paranoia or delusions in some cases
Physical Symptoms
- Walking problems: a slow, shuffling gait or balance difficulties
- Weakness or numbness in limbs, especially following a stroke
- Urinary incontinence or urgency
- Falls
- Dizziness
How Symptoms Appear Over Time
One distinctive feature of vascular dementia — particularly the multi-infarct type — is that symptoms often appear suddenly following a stroke or TIA, then plateau for a period, then worsen again with another vascular event. This “stepwise” progression is different from the gradual, nearly imperceptible decline typically seen in Alzheimer’s disease. In small vessel disease, however, decline may be slow and steady rather than stepwise.
Stages of Vascular Dementia
Vascular dementia does not follow a perfectly uniform staging pathway the way some other dementias do, because its progression depends heavily on whether further vascular events occur. That said, clinicians generally describe the condition in three broad stages.
| Stage | Typical Characteristics | Daily Function |
|---|---|---|
| Early Stage | Mild memory lapses, subtle difficulty with complex tasks, slowed thinking, possible mood changes or depression | Person can generally manage daily activities with some effort; may need reminders or help with complex tasks like finances |
| Middle Stage | More noticeable memory problems, confusion, significant difficulty with planning and reasoning, behavioral changes, possible walking or balance issues | Increasing need for assistance with daily activities; may become unsafe alone; communication difficulties worsen |
| Late Stage | Severe cognitive impairment, inability to recognize familiar people, loss of communication, significant physical decline, incontinence | Full-time care required; person is largely dependent for all activities of daily living |
Some people with vascular dementia — especially those whose vascular risk factors are well managed — experience slower progression than others. Preventing additional strokes or vascular events is the most important way to slow the course of the disease.
Vascular Dementia vs. Alzheimer’s Disease
People often ask how vascular dementia is different from Alzheimer’s disease. The two conditions are related — and frequently overlap — but they have distinct origins and patterns.
| Feature | Vascular Dementia | Alzheimer’s Disease |
|---|---|---|
| Primary cause | Reduced or blocked blood flow to the brain | Buildup of amyloid plaques and tau tangles in brain tissue |
| Onset | Often sudden (after stroke) or stepwise | Gradual and insidious |
| Early symptoms | Executive function problems (planning, reasoning) | Memory problems (especially recent events) |
| Progression | Stepwise (worsens after vascular events) or slow and steady | Slow, continuous decline |
| Physical symptoms | Common early (gait problems, weakness) | Usually appear later in the disease |
| Depression | Very common | Common but slightly less prominent early on |
| Brain imaging findings | Evidence of strokes, white matter changes, reduced blood flow | Brain atrophy, particularly in hippocampus |
| Risk factor overlap | Strong overlap with cardiovascular risk factors | Some overlap; also age, genetics (APOE ε4) |
| Potentially preventable? | Significantly, through vascular risk factor control | Partially, through lifestyle measures |
Mixed dementia — where both vascular damage and Alzheimer’s pathology are present — is actually quite common, particularly in older adults. Research suggests that up to 45% of people with dementia may have a mixed form, according to the Alzheimer’s Association.
How Is Vascular Dementia Diagnosed?
There is no single test that diagnoses vascular dementia. Instead, diagnosis involves a combination of medical history, physical examination, cognitive testing, and brain imaging. A thorough evaluation is important because many conditions can cause cognitive symptoms, and identifying the underlying cause guides treatment decisions.
Medical History and Physical Examination
The doctor will ask detailed questions about when symptoms started, how they have changed over time, any history of stroke or TIA, and cardiovascular risk factors. A complete neurological exam will check reflexes, coordination, balance, and motor function for signs consistent with vascular damage.
Cognitive and Neuropsychological Testing
Standardized tests assess memory, attention, language, visuospatial skills, and executive function. It can also include the Montreal Cognitive Assessment (MoCA) and also – Mini-Mental State Examination (MMSE). More extensive neuropsychological batteries may be used to map the specific pattern of cognitive strengths and weaknesses.
Brain Imaging
Brain imaging is essential in diagnosing vascular dementia. It can reveal evidence of past strokes, areas of reduced blood flow, and white matter changes that support a vascular cause.
| Imaging Type | What It Shows | Role in Diagnosis |
|---|---|---|
| MRI (Magnetic Resonance Imaging) | Detailed images of brain tissue; shows white matter lesions, infarcts, atrophy | Primary imaging tool; most sensitive for vascular changes |
| CT Scan (Computed Tomography) | Structural brain images; shows large strokes, hemorrhage, atrophy | Often used initially; less sensitive than MRI for small vessel changes |
| PET Scan | Shows patterns of brain metabolism and blood flow | Useful to distinguish vascular from Alzheimer’s dementia in complex cases |
| Carotid Ultrasound | Images carotid arteries for narrowing or plaque | Assesses stroke risk and vascular health |
Laboratory Tests
Blood tests rule out other treatable causes of cognitive decline, such as thyroid disorders, vitamin B12 deficiency, kidney or liver disease, infections, and anemia. These tests are a routine part of any dementia workup.
Cardiovascular Evaluation
Because vascular dementia is closely tied to heart and blood vessel health, an electrocardiogram (ECG) may be performed to check for atrial fibrillation or other cardiac conditions that increase stroke risk. Blood pressure measurement is always a key part of the evaluation.
Treatment of Vascular Dementia
It is honest and important to tell you directly: there is currently no medication approved specifically to treat or reverse vascular dementia. However, this does not mean nothing can be done. Treatment focuses on two major goals — preventing further vascular damage and managing symptoms — and in both areas, there is a great deal that medicine and lifestyle can offer.
Preventing Further Vascular Events
The most important treatment for vascular dementia is preventing additional strokes and vascular injury. Each new stroke event can cause further cognitive decline, so controlling the underlying risk factors is the most powerful intervention available. According to the National Heart, Lung, and Blood Institute (NHLBI) and NINDS, the following measures are central to management:
| Treatment Target | Approach | Goal |
|---|---|---|
| High blood pressure | Antihypertensive medications (ACE inhibitors, ARBs, calcium channel blockers, diuretics); dietary changes; exercise | Maintain blood pressure below 130/80 mmHg (per current guidelines) |
| High cholesterol | Statins (e.g., atorvastatin, rosuvastatin); dietary changes | Reduce LDL cholesterol; protect blood vessel walls |
| Diabetes management | Blood sugar medications; insulin; diet; exercise | Maintain stable blood glucose levels to protect blood vessels |
| Atrial fibrillation | Anticoagulant medications (e.g., warfarin, apixaban, rivaroxaban); rate control medications | Prevent blood clots that can travel to the brain |
| Blood clot prevention (after ischemic stroke or TIA) | Antiplatelet medications (aspirin, clopidogrel) | Reduce risk of future stroke |
| Smoking cessation | Counseling, nicotine replacement, prescription medications (varenicline, bupropion) | Eliminate one of the most significant vascular risk factors |
| Carotid artery disease | Carotid endarterectomy or stenting if significant narrowing is present | Restore blood flow and prevent stroke |
Medications for Cognitive Symptoms
While no medications are specifically approved by the FDA for vascular dementia, some doctors prescribe medications used in Alzheimer’s disease to help manage cognitive symptoms in vascular dementia, particularly when mixed dementia is present or suspected. The evidence is modest but some patients experience benefit.
| Medication Class | Examples | Potential Role |
|---|---|---|
| Cholinesterase inhibitors | Donepezil (Aricept), rivastigmine (Exelon), galantamine (Razadyne) | May modestly improve or stabilize cognitive symptoms; more evidence in mixed dementia |
| NMDA receptor antagonist | Memantine (Namenda) | May help with cognitive symptoms in moderate to severe disease; sometimes used off-label |
Always discuss the potential benefits and risks of these medications with a physician who knows your full medical history. Not every person with vascular dementia will be a candidate for these treatments.
Managing Behavioral and Psychological Symptoms
Depression is particularly common in vascular dementia and should always be treated. Antidepressants, particularly SSRIs (selective serotonin reuptake inhibitors) such as sertraline or citalopram, are often used. They tend to be well tolerated in older adults and can significantly improve quality of life.
Anxiety, agitation, and sleep disturbances may also require treatment. Non-drug approaches — structured routines, a calm environment, meaningful activities — are always tried first. Medications are used when behavioral symptoms are causing significant distress or safety concerns, and only at the lowest effective dose.
Lifestyle That Can Help With Vascular Dementia
Lifestyle changes play a meaningful role not only in preventing vascular dementia but also in slowing its progression and improving overall wellbeing. The following are supported by evidence from leading health organizations including the Centers for Disease Control and Prevention (CDC) and the National Institutes of Health (NIH).
Physical Exercise
Regular physical activity benefits the brain directly by improving blood flow, reducing blood pressure, lowering blood sugar, and supporting the growth of new brain connections. Aim for at least 150 minutes of moderate-intensity aerobic activity per week (such as brisk walking, swimming, or cycling), as recommended by the CDC. Even shorter bouts of activity throughout the day add up and are beneficial.
Heart-Healthy Diet
A diet that protects your heart also protects your brain. The DASH diet (Dietary Approaches to Stop Hypertension) and the Mediterranean diet are both strongly supported by research for reducing cardiovascular risk. Key principles include: plenty of vegetables and fruits; whole grains over refined grains; lean protein sources including fish; healthy fats (olive oil, nuts, avocado); and limiting sodium, saturated fats, added sugars, and processed foods.
Not Smoking
Smoking damages blood vessels throughout the body, increases blood clotting, raises blood pressure, and significantly increases stroke risk. Quitting smoking at any age reduces these risks. Your doctor can connect you with resources and medications to help.
Limiting Alcohol
Heavy alcohol use raises blood pressure and increases stroke risk. The Dietary Guidelines for Americans recommend no more than one drink per day for women and two for men — and less is better when brain health is the goal.
Managing Stress
Chronic stress is associated with elevated blood pressure and inflammation, both of which affect vascular health. Techniques such as relaxation breathing, mindfulness, gentle yoga, and maintaining social connections can all help manage stress levels.
Cognitive and Social Engagement
Staying mentally active — reading, learning new skills, engaging in hobbies — and maintaining social connections may support brain resilience. While these activities cannot undo vascular damage, they may help maintain function and quality of life.
Monitoring and Managing Sleep
Untreated sleep apnea (where breathing repeatedly stops during sleep) strains the cardiovascular system and reduces oxygen delivery to the brain during the night. If you or someone you care for snores heavily, gasps during sleep, or wakes feeling unrefreshed, mention this to a doctor. Treatment of sleep apnea with CPAP (continuous positive airway pressure) therapy can meaningfully improve cardiovascular outcomes.
Caring for Someone with Vascular Dementia
If you are a caregiver for someone with vascular dementia, your role is genuinely important — and it can also be genuinely hard. Here are some approaches that many caregivers and care teams have found helpful.
Creating a Safe Environment
As vascular dementia progresses, safety becomes a growing concern. Balance problems and gait difficulties increase fall risk. Consider removing loose rugs, installing grab bars in bathrooms, improving lighting throughout the home, and placing safety locks on doors and cabinets where necessary. A home safety evaluation by an occupational therapist can identify risks specific to your home.
Establishing Routine
People with dementia generally do better with predictable, structured days. Consistent mealtimes, activity times, and sleep schedules reduce confusion and anxiety. Sudden changes in routine or environment can trigger agitation or disorientation.
Communication Strategies
Speak slowly and clearly, using short sentences. Allow time for the person to process what you have said before repeating or responding. Reduce distracting noise or activity in the background. If they cannot find a word, offer gentle help rather than finishing sentences for them unless they want that.
Caregiver Wellbeing
Caregiver burnout is real, and it matters — both for you and for the person you are caring for. Reaching out for help is not a sign of weakness; it is a sign that you understand the demands of the situation. Respite care, support groups, and counseling services are available in most communities. The Alzheimer’s Association (alz.org) and the Caregiver Action Network offer resources specifically for dementia caregivers.
When to Seek Medical Attention
Some situations require prompt medical attention and should not be waited out. Seek emergency care immediately if you notice any of the following, which may signal a stroke or TIA:
-
- Numbness or weakness that comes on abruptly in the face, an arm, or a leg — particularly when it affects only one side of the body
- Abrupt confusion, difficulty getting words out, or trouble making sense of what others are saying
- Vision that suddenly goes blurry, doubles, or disappears in one or both eyes
- A severe headache that strikes without warning and has no obvious explanation
- Abrupt loss of balance, unsteadiness on the feet, or a sudden inability to coordinate movement
The acronym FAST — Face drooping, Arm weakness, Speech difficulty, Time to call 911 — is a quick way to remember the warning signs of stroke. Acting quickly dramatically improves outcomes. Every minute counts when a stroke is occurring.
Outside of emergencies, schedule an appointment with a doctor if you notice gradual cognitive changes in yourself or a loved one, even if they seem mild. Early evaluation allows for earlier intervention, treatment of reversible causes, and better planning for the future.
Prognosis and Life Expectancy
The outlook for someone with vascular dementia varies considerably depending on the underlying cause, the extent of brain damage, age, general health, and — critically — whether further vascular events are prevented.
People with vascular dementia who are otherwise healthy, who successfully manage their cardiovascular risk factors, and who do not experience additional strokes can live for many years with the condition. Some research suggests that people with vascular dementia have shorter average life expectancies than their peers, largely because the underlying vascular disease also affects the heart and other organs — not because the dementia itself is typically the direct cause of death.
Vascular dementia is one of the dementias most amenable to modification through treatment and lifestyle. This does not mean it is curable, but it does mean that the choices made in terms of blood pressure control, medication adherence, diet, and exercise can genuinely affect how the condition progresses.
Frequently Asked Questions About Vascular Dementia
Is vascular dementia hereditary?
In most cases of vascular dementia result from a lifetime accumulation of vascular risk factors — high blood pressure, diabetes, smoking — rather than genetics. However, some forms, like CADASIL, are directly caused by a genetic mutation and run strongly in families. A family history of early stroke or young-onset dementia warrants a conversation with a doctor about genetic counseling.
Can vascular dementia be reversed?
The brain damage caused by past strokes or vascular events cannot be reversed. However, further decline can often be slowed or stabilized by preventing new vascular events. Some symptoms — particularly those related to depression, medication side effects, or poorly controlled blood pressure — may improve with appropriate treatment.
How is vascular dementia different from normal aging?
Normal aging may bring some slowing of processing speed and occasional forgetfulness — for example, occasionally forgetting a name and remembering it later. Vascular dementia involves changes that are more significant, more consistent, and that interfere with daily functioning. If cognitive changes are noticeable, persistent, or affecting independence or safety, they should be evaluated by a doctor.
What is the difference between a TIA and a stroke?
A transient ischemic attack (TIA) causes the same symptoms as a stroke — sudden weakness, numbness, speech problems — but symptoms resolve completely within 24 hours (usually within an hour). A TIA should be treated as a serious warning sign. People who have a TIA have a significantly elevated risk of having a full stroke within days to weeks, and prompt medical evaluation is essential.
Should family members get tested if a relative has CADASIL?
CADASIL is caused by a dominant gene mutation, meaning first-degree relatives of someone diagnosed with CADASIL have a 50% chance of carrying the mutation. Genetic testing is available. Families dealing with possible CADASIL should be referred to a neurologist with expertise in the condition and ideally to a genetic counselor who can help them understand the implications of testing.
What support services are available?
People living with vascular dementia and their families do not have to figure everything out alone. Support comes in many forms — neurologists and memory care specialists for medical guidance, social workers for help with care planning and financial questions, home health aides for day-to-day assistance, adult day programs for structured activity and social connection, and respite care for family caregivers who need a break. Peer support groups, both in-person and online, can also make a real difference. The Alzheimer’s Association operates a around-the-clock helpline at 1-800-272-3900 and maintains a searchable directory of local services throughout the United States.
Suggested Sources
- National Institute of Neurological Disorders and Stroke (NINDS)
NINDS Vascular Dementia Information - American Heart Association/American Stroke Association (AHA/ASA)
AHA/ASA Vascular Contributions to Cognitive Impairment and Dementia - Alzheimer’s Association
Alzheimer’s Association: Vascular Dementia
What helped us to write this article
- Bondi, M.W. and Edmonds, E.C. (2022) ‘Dementia: Clinical features, assessment, and diagnosis’, The Lancet, 400(10348), pp. 1821–1834.
- Gorelick, P.B. et al. (2011) ‘Vascular contributions to cognitive impairment and dementia: A statement for healthcare professionals from the American Heart Association/American Stroke Association’, Stroke, 42(9), pp. 2672–2713.
- Kalaria, R.N. (2016) ‘Neuropathological diagnosis of vascular cognitive impairment and vascular dementia with implications for Alzheimer’s disease’, Acta Neuropathologica, 131(5), pp. 659–685.
- Lopez, O.L. et al. (2005) ‘Prevalence and classification of mild cognitive impairment in the Cardiovascular Health Study–Cognition Study’, Archives of Neurology, 62(3), pp. 411–414.
- O’Brien, J.T. and Thomas, A. (2015) ‘Vascular dementia’, Lancet, 386(10004), pp. 1698–1706.
- Roman, G.C. et al. (1993) ‘Vascular dementia: Diagnostic criteria for research studies. Report of the NINDS–AIREN International Workshop’, Neurology, 43(2), pp. 250–260.
- Skrobot, O.A. et al. (2018) ‘Vascular cognitive impairment and dementia: A practical guide for clinicians’, Journal of Neurology, Neurosurgery & Psychiatry, 89(6), pp. 688–696.
- Smith, E.E. (2017) ‘Clinical presentations and epidemiology of vascular dementia’, Clinical Science, 131(11), pp. 1059–1068.
- Winblad, B. et al. (2004) ‘Mild cognitive impairment—beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment’, Journal of Internal Medicine, 256(3), pp. 240–246.
- Yoshita, M. et al. (2006) ‘White matter hyperintensities and cerebral microbleeds: Markers of vascular brain injury in dementia’, Annals of the New York Academy of Sciences, 977(1), pp. 89–99.